
CrashDuringApproachtoLanding
EmpireAirlinesFlight8284
AvionsdeTransportRégional
AerospatialeAleniaATR42‐320,N902FX
Lubbock,Texas
January27,2009
Accident Report
NTSB/AAR-11/02
PB2011-910402
National
Transportation
Safety Board
NTSB/AAR-11/02
PB2011-910402
Notation 8093A
Adopted April 26, 2011
Aircraft Accident Report
Crash During Approach to Landing
Empire Airlines Flight 8284
Avions de Transport Régional
Aerospatiale Alenia ATR 42-320, N902FX
Lubbock, Texas
January 27, 2009
National
Transportation
Safety Board
490 L’Enfant Plaza, S.W.
Washington, D.C. 20594

National Transportation Safety Board. 2011. Crash During Approach to Landing, Empire Airlines
Flight 8284, Avions de Transport Régional Aerospatiale Alenia ATR 42-320, N902FX, Lubbock,
Texas, January 27, 2009. Aircraft Accident Report NTSB/AAR-11/02. Washington, DC.
Abstract: This accident report discusses the January 27, 2009, accident involving Empire Airlines
flight 8284, an Avions de Transport Régional Aerospatiale Alenia ATR 42-320, N902FX, which crashed
short of the runway at Lubbock Preston Smith International Airport, Lubbock, Texas. The captain
sustained serious injuries, and the first officer sustained minor injuries. The airplane was substantially
damaged. The airplane was registered to FedEx Corporation and operated by Empire Airlines, Inc., as a
14 Code of Federal Regulations Part 121 supplemental cargo flight. Instrument meteorological conditions
prevailed, and an instrument flight rules flight plan was filed. The safety issues discussed in this report
include the flight crew’s actions in response to the flap anomaly, the continuation of the unstabilized
approach, the dispatch of the flight into freezing drizzle conditions, the efficiency of the emergency
response, and simulator-based training for pilots who fly in icing conditions. Nine safety
recommendations are addressed to the Federal Aviation Administration.
The National Transportation Safety Board is an independent Federal agency dedicated to promoting aviation,
railroad, highway, marine, pipeline, and hazardous materials safety. Established in 1967, the agency is mandated by
Congress through the Independent Safety Board Act of 1974 to investigate transportation accidents, determine the
probable causes of the accidents, issue safety recommendations, study transportation safety issues, and evaluate the
safety effectiveness of government agencies involved in transportation. The Safety Board makes public its actions
and decisions through accident reports, safety studies, special investigation reports, safety recommendations, and
statistical reviews.
Recent publications are available in their entirety on the Internet at <http://www.ntsb.gov>. Other information about
available publications also may be obtained from the website or by contacting:
National Transportation Safety Board
Records Management Division, CIO-40
490 L’Enfant Plaza, SW
Washington, DC 20594
(800) 877-6799 or (202) 314-6551
Safety Board publications may be purchased, by individual copy or by subscription, from the National Technical
Information Service. To purchase this publication, order report number PB2011-910402 from:
National Technical Information Service
5285 Port Royal Road
Springfield, Virginia 22161
(800) 553-6847 or (703) 605-6000
The Independent Safety Board Act, as codified at 49 U.S.C. Section 1154(b), precludes the admission into evidence
or use of Board reports related to an incident or accident in a civil action for damages resulting from a matter
mentioned in the report.

NTSB Aircraft Accident Report
Contents
Figures ........................................................................................................................................... iv
Abbreviations and Acronyms .......................................................................................................v
Executive Summary ..................................................................................................................... ix
1. Factual Information ...................................................................................................................1
1.1 History of Flight .........................................................................................................................1
1.2 Injuries to Persons ......................................................................................................................5
1.3 Damage to Airplane ...................................................................................................................5
1.4 Other Damage ............................................................................................................................5
1.5 Personnel Information ................................................................................................................6
1.5.1 The Captain ......................................................................................................................6
1.5.2 The First Officer ..............................................................................................................6
1.5.3 Flight Crew’s Rest Opportunities ....................................................................................7
1.5.3.1 The Captain ....................................................................................................... 7
1.5.3.2 The First Officer ............................................................................................... 8
1.6 Airplane Information .................................................................................................................8
1.6.1 General .............................................................................................................................8
1.6.2 Flap System .....................................................................................................................9
1.6.3 Deicing, Anti-Icing, and Anti-Icing Advisory Systems ................................................11
1.6.4 Flight Instruments ..........................................................................................................11
1.6.4.1 Airspeed Indicator ........................................................................................... 11
1.6.4.2 Electronic Flight Information System ............................................................. 13
1.6.5 Automatic Flight Control System ..................................................................................13
1.6.6 Stall Protection System ..................................................................................................13
1.7 Meteorological Information .....................................................................................................14
1.8 Aids to Navigation ...................................................................................................................14
1.9 Communications ......................................................................................................................15
1.10 Airport Information ................................................................................................................15
1.10.1 Emergency Plan ...........................................................................................................15
1.10.2 Snow and Ice Control Plan ..........................................................................................16
1.11 Flight Recorders .....................................................................................................................16
1.11.1 Cockpit Voice Recorder ..............................................................................................16
1.11.2 Flight Data Recorder ....................................................................................................17
1.12 Wreckage and Impact Information ........................................................................................17
1.13 Medical and Pathological Information ...................................................................................18
1.14 Fire .........................................................................................................................................18
1.15 Survival Aspects ....................................................................................................................18
1.15.1 Flight Crew Egress ......................................................................................................18
1.15.2 Emergency Response ...................................................................................................18
1.16 Tests and Research .................................................................................................................21
1.16.1 Airplane Performance Study and Simulator Evaluations ............................................21
i

NTSB Aircraft Accident Report
1.16.1.1 Effects of Flap Asymmetry ........................................................................... 21
1.16.1.2 Effects of Airframe Ice Accretion ................................................................. 22
1.16.2 Terrain Awareness and Warning System ....................................................................23
1.16.3 Flap System Component Examinations .......................................................................24
1.16.3.1 Hydraulic Fluid Testing ................................................................................ 25
1.16.3.2 Maintenance History ..................................................................................... 25
1.16.3.3 Flap Asymmetry Event Involving Another Airplane .................................... 25
1.16.4 Deicing and Anti-Icing System Examinations ............................................................26
1.16.5 Autopilot Disconnect Alert ..........................................................................................26
1.17 Organizational and Management Information .......................................................................26
1.17.1 Pilot Standard Operating Procedures and Training .....................................................27
1.17.1.1 Flap Anomalies ............................................................................................. 27
1.17.1.2 Stabilized Approach and Go Around ............................................................ 31
1.17.1.3 Terrain Awareness and Warning System ...................................................... 32
1.17.1.4 Airspeed Bugs ............................................................................................... 32
1.17.1.5 Aileron Mistrim with Autopilot Engaged ..................................................... 33
1.17.1.6 Deicing and Anti-Icing Systems ................................................................... 33
1.17.1.7 Crew Resource Management ........................................................................ 34
1.17.1.8 Weather Information and Training ............................................................... 35
1.17.1.9 Stall and Near-Stall Recoveries .................................................................... 36
1.17.2 Aircraft Deicing Program (Ground) ............................................................................36
1.17.3 Flight Dispatch .............................................................................................................36
1.17.4 Hazardous Materials ....................................................................................................38
1.17.5 Federal Aviation Administration Oversight ................................................................38
1.17.6 Previous Accidents ......................................................................................................39
1.18 Additional Information ..........................................................................................................40
1.18.1 Postaccident Safety Action ..........................................................................................40
1.18.1.1 Federal Aviation Administration .................................................................. 40
1.18.1.2 Empire Airlines ............................................................................................. 41
1.18.1.3 FedEx Feeder Operations .............................................................................. 42
1.18.2 Previously Issued Safety Recommendations ...............................................................43
1.18.2.1 Flight Crew Monitoring and Workload Management Skills for Single and
Multiple Abnormal Situations..................................................................................... 43
1.18.2.2 Go-Around Callout ....................................................................................... 45
1.18.2.3 Low-Airspeed Alerting Systems ................................................................... 45
1.18.2.4 First Officer Assertiveness ............................................................................ 46
1.18.3 Airplane Equipment Options .......................................................................................47
1.18.3.1 Aircraft Performance Monitoring System .................................................... 47
1.18.3.2 Flap Malfunction or Asymmetry Light ......................................................... 48
1.18.3.3 Ice Evidence Probe ....................................................................................... 49
2. Analysis .....................................................................................................................................50
2.1 General .....................................................................................................................................50
2.2 Accident Sequence ...................................................................................................................52
2.3 Human Performance ................................................................................................................54
2.3.1 Captain’s Nonstandard Responses .................................................................................55
2.3.2 Flight Crew’s Failure to Monitor Airspeed ...................................................................57
ii

NTSB Aircraft Accident Report
2.3.2.1 Airspeed References ....................................................................................... 58
2.3.2.2 Flight Crew Monitoring Skills and Techniques .............................................. 60
2.3.3 Crew Resource Management .........................................................................................61
2.3.4 Go-Around Callout ........................................................................................................63
2.3.5 Training for Single and Multiple Abnormal Situations Occurring at Low Altitude .....64
2.3.6 Fatigue Considerations ..................................................................................................65
2.3.6.1 Role of Fatigue in Flight Crew Performance .................................................. 67
2.4 Operations Issues .....................................................................................................................69
2.4.1 Dispatch into Freezing Drizzle Conditions ....................................................................69
2.4.1.1 Flight Crewmember and Dispatcher Training Related to Icing Conditions ... 70
2.4.1.2 Proposed Rulemaking for Airplane Certification Requirements for Flight in
Icing Conditions .......................................................................................................... 72
2.4.2 Training Program and Manual Discrepancies ...............................................................72
2.5 Survival Aspects ......................................................................................................................73
2.5.1 Lack of Occupant and Hazardous Materials Information Available
to First Responders .................................................................................................................73
2.5.2 Inoperative Emergency Response and Mutual Aid Gate ...............................................75
2.6 Airplane Equipment Options ...................................................................................................75
2.6.1 Aircraft Performance Monitoring ..................................................................................75
2.6.2 Flap Malfunction or Asymmetry Light ..........................................................................77
2.6.3 Ice Evidence Probe ........................................................................................................77
2.7 Simulator Training for Icing Encounters .................................................................................78
3. Conclusions ...............................................................................................................................80
3.1 Findings....................................................................................................................................80
3.2 Probable Cause.........................................................................................................................83
4. Recommendations ....................................................................................................................84
Board Member Statements .........................................................................................................86
5. Appendixes ...............................................................................................................................93
Appendix A: Investigation and Hearing ........................................................................................93
Appendix B: Cockpit Voice Recorder Transcript ..........................................................................94
iii

NTSB Aircraft Accident Report
Figures
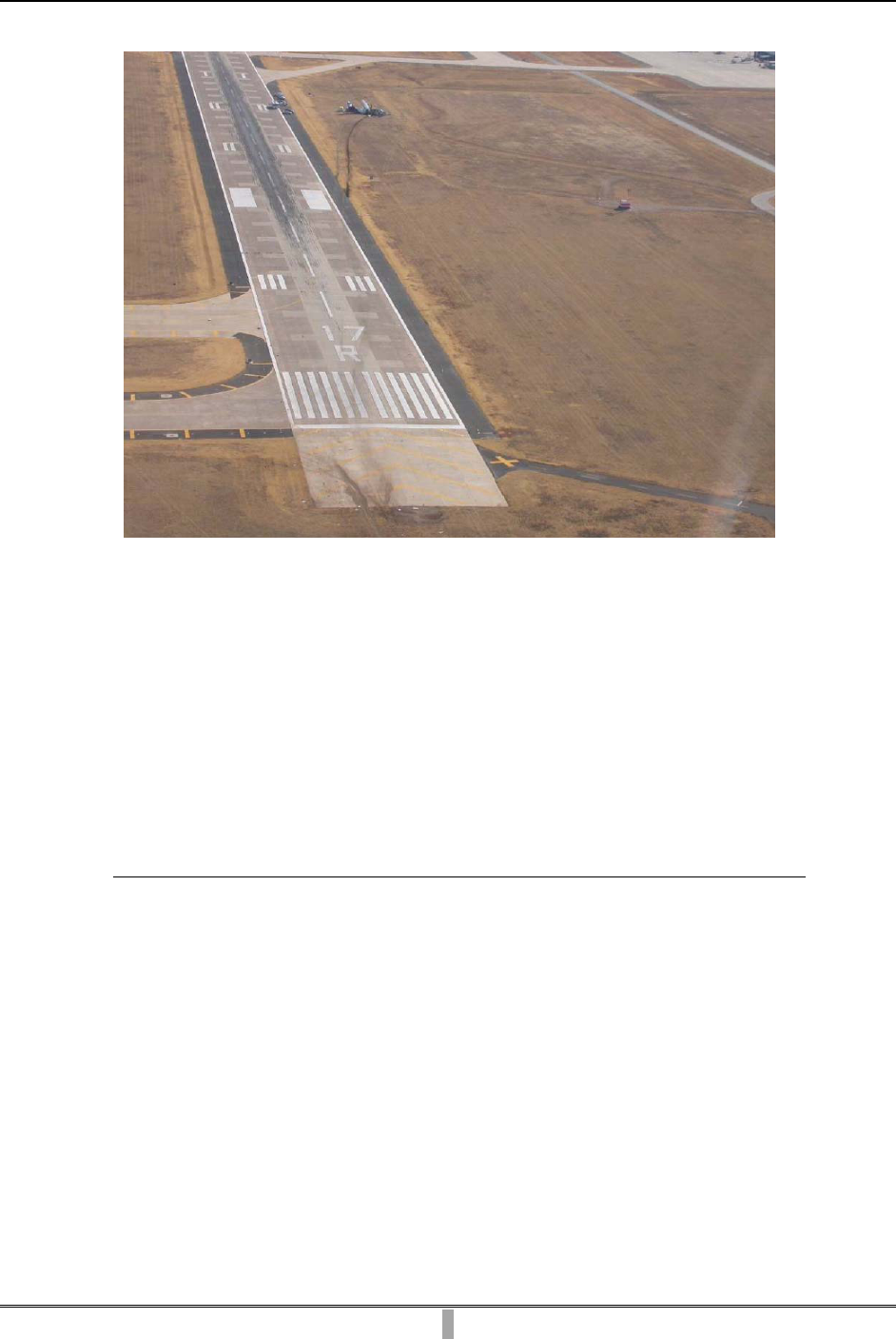
Figure 1. Aerial view of approach end of runway 17R and location of wreckage. ....................... 5
Figure 2. Flap position indicator. Inset shows the likely needle pointer position during the
flap asymmetry.............................................................................................................................. 10
Figure 3. Exterior flap position fairing. ....................................................................................... 10
Figure 4. Airspeed indicator showing needle pointer; selector knob; and internal, yellow,
white, and red bugs. ...................................................................................................................... 12
Figure 5. View of airport showing relative locations of airport access gates and accident site. . 20
Figure 6. Right side of fuselage showing extensive fire damage to right wing and
flap components. ........................................................................................................................... 24
Figure 7. Quick reference handbook page 2.21 with “FLAPS JAM/UNCOUPLED/ASYM” and
“REDUCED FLAPS LANDING” procedures. ............................................................................ 28
Figure 8. General information on page 0.02 of quick reference handbook. ................................ 29
iv

NTSB Aircraft Accident Report
Abbreviations and Acronyms
AAS anti-icing advisory system
AC advisory circular
AD airworthiness directive
ADP aircraft deicing program
ADU advisory display unit
AEP airport emergency plan
AFFF aqueous film forming foam
AFM airplane flight manual
AFW Fort Worth Alliance Airport
agl above ground level
AIM Aeronautical Information Manual
AIRMET airmen’s meteorological information
AOA angle of attack
APM aircraft performance monitoring
ARAC Aviation Rulemaking Advisory Committee
ARFF aircraft rescue and firefighting
ATC air traffic control
ATCT air traffic control tower
ATOS air transportation oversight system
ATR Avions de Transport Régional
ATR 42 Aerospatiale Alenia ATR 42-320
BEA Bureau d’Enquêtes et d’Analyses
CFR Code of Federal Regulations
v

NTSB Aircraft Accident Report
CG center of gravity
CRM crew resource management
CVR cockpit voice recorder
DGAC Direction Générale de l’Aviation Civile
EADI electronic attitude direction indicator
EASA European Aviation Safety Agency
EFS engineering flight simulator
ELP El Paso International Airport
EMS emergency medical service
FAA Federal Aviation Administration
FAF final approach fix
FCOM flight crew operating manual
FDR flight data recorder
FedEx FedEx Corporation
FL flight level
fpm feet per minute
FR Federal Register
FSDO flight standards district office
FSIB flight standards information bulletin
FTM flight training manual
GOM general operations manual
HAZMAT hazardous materials
Hg mercury
IEP ice evidence probe
vi
NTSB Aircraft Accident Report
IFR instrument flight rules
ILS instrument landing system
IMC instrument meteorological conditions
InFO information for operators
KIAS knots indicated airspeed
kts knots
LBB Lubbock Preston Smith International Airport
lbs pounds
LOM locator outer marker
LWD left-wing-down
MAF Midland International Airport
msl mean sea level
NASA National Aeronautics and Space Administration
NPRM notice of proposed rulemaking
NTSB National Transportation Safety Board
NWS National Weather Service
PF pilot flying
PIC pilot-in-command
PM pilot monitoring
PMI principal maintenance inspector
POI principal operations inspector
QRH quick reference handbook
RWD right-wing-down
SAFO safety alert for operators
SIC second-in-command
vii

NTSB Aircraft Accident Report
SIGMET significant meteorological information
SLD supercooled large droplet
SN serial number
SOP standard operating procedure
STC supplemental type certificate
SVFR special visual flight rules
TAWS terrain awareness and warning system
TSB Transportation Safety Board of Canada
VFR visual flight rules
V
ga
minimum approach airspeed for 30° flaps plus 5 kts (not corrected for wind) or
1.1 V
mca
, whichever is greater
V
mca
minimum control airspeed with 5° of bank and the failure of the critical engine
with takeoff flaps and landing gear retracted
V
mHB
30 minimum approach airspeed and target touchdown airspeed with 30° flaps
V
mLB
0
minimum approach airspeed for 0° flaps
VMC visual meteorological conditions
viii

NTSB Aircraft Accident Report
ix
Executive Summary
On January 27, 2009, about 0437 central standard time, an Avions de Transport Régional
Aerospatiale Alenia ATR 42-320, N902FX, operating as Empire Airlines flight 8284, was on an
instrument approach when it crashed short of the runway at Lubbock Preston Smith International
Airport, Lubbock, Texas. The captain sustained serious injuries, and the first officer sustained
minor injuries. The airplane was substantially damaged. The airplane was registered to FedEx
Corporation and operated by Empire Airlines, Inc., as a 14 Code of Federal Regulations Part 121
supplemental cargo flight. The flight departed from Fort Worth Alliance Airport, Fort Worth,
Texas, about 0313. Instrument meteorological conditions prevailed, and an instrument flight
rules flight plan was filed.
The National Transportation Safety Board determines that the probable cause of this
accident was the flight crew’s failure to monitor and maintain a minimum safe airspeed while
executing an instrument approach in icing conditions, which resulted in an aerodynamic stall at
low altitude. Contributing to the accident were 1) the flight crew’s failure to follow published
standard operating procedures in response to a flap anomaly, 2) the captain’s decision to
continue with the unstabilized approach, 3) the flight crew’s poor crew resource management,
and 4) fatigue due to the time of day in which the accident occurred and a cumulative sleep debt,
which likely impaired the captain’s performance.
The safety issues discussed in this report include the flight crew’s actions in response to
the flap anomaly, the continuation of the unstabilized approach, the dispatch of the flight into
freezing drizzle conditions, the efficiency of the emergency response, and simulator-based
training for pilots who fly in icing conditions. Nine safety recommendations are addressed to the
Federal Aviation Administration.

NTSB Aircraft Accident Report
1
1. Factual Information
1.1 History of Flight
On January 27, 2009, about 0437 central standard time,
1
an Avions de Transport
Régional (ATR) Aerospatiale Alenia ATR 42-320 (ATR 42), N902FX, operating as Empire
Airlines flight 8284, was on an instrument approach when it crashed short of the runway at
Lubbock Preston Smith International Airport (LBB), Lubbock, Texas. The captain sustained
serious injuries, and the first officer sustained minor injuries. The airplane was substantially
damaged. The airplane was registered to FedEx Corporation (FedEx) and operated by Empire
Airlines, Inc., as a 14 Code of Federal Regulations (CFR) Part 121 supplemental cargo flight.
The flight departed from Fort Worth Alliance Airport (AFW), Fort Worth, Texas, about 0313.
Instrument meteorological conditions (IMC) prevailed,
2
and an instrument flight rules (IFR)
flight plan was filed.
During the flight’s initial descent to LBB, the first officer was the pilot flying (PF) with
the autopilot system engaged. As the airplane descended from 14,000 to 8,000 feet above mean
sea level (msl), the captain, who was the pilot monitoring (PM), performed the descent and
approach checklists. Review of the cockpit voice recorder (CVR) transcript revealed that the
captain confirmed that the airplane’s anti-icing and deicing protection was set to level 3.
3
The
captain performed the approach briefing,
4
which included what he believed to be the “icing
speed” information (minimum maneuvering and operating airspeeds for approach in icing
conditions).
5
According to the CVR transcript, at 0419:41, the captain briefed the first officer about the
missed approach procedure for the instrument landing system (ILS) approach to runway 17R,
6
stating that “in the event of a miss it’ll be uh climb to thirty seven and a right turn to five
1
All times in this report are central standard time (unless otherwise noted) and based on a 24-hour clock.
2
According to the Federal Aviation Administration (FAA) Pilot/Controller Glossary, IMC is defined as
“meteorological conditions expressed in terms of visibility, distance from cloud, and ceiling [that are] less than the
[minimums] specified for visual meteorological conditions.” At the time of the accident airplane’s approach, LBB’s
ceiling and visibility were below the minimums specified in 14 CFR 91.155 for flight under visual flight rules.
Information obtained from the FAA’s website <http://www.faa.gov/air_traffic/publications/atpubs/PCG/> (accessed
March 21, 2011).
3
The airplane flight manual contained guidelines for using the anti-icing and deicing systems. For more
information, see section 1.17.1.6.
4
During postaccident interviews, the flight crewmembers reported that the captain performed the approach
briefing because they anticipated that he would be flying the approach. They believed that weather conditions were
at the minimums for the approach (ceiling 200 feet above ground level, visibility 1/2 mile), and they were unsure if
the first officer had accumulated the 100 hours of flight time in the ATR 42 required by Empire Airlines for her to
fly the approach to minimums. Subsequently, they learned that the weather conditions were above minimums and
decided that the first officer would fly the approach.
5
For more information about the captain’s approach airspeed briefing and the flight crew’s procedures for
obtaining and using such information, see section 1.17.1.4.
6
According to the CVR transcript, the air traffic controller informed the flight crew that runway 8/26 was
closed and that the localizer back course approach, which the first officer recognized as the only approach for
runway 35L, was unavailable. The flight crew discussed that the winds were from the north but that runway 17R
was the only available option.
NTSB Aircraft Accident Report
2
hundred feet
[7]
via the Lubbock one fourteen radial to HYDRO intersection and hold annnd
[8]
that looks like a parallel entry.” The first officer acknowledged this statement, and the captain
then stated, “climb to thirty seven and a left turn to five out to one fourteen.”
At 0422:32, the LBB approach controller cleared the flight to descend to 6,000 feet msl
and advised that he had not received any icing reports and that the special weather observation
about 0408 indicated winds from 350° at 10 knots (kts), visibility 2 miles in light freezing drizzle
and mist, ceiling overcast at 500 feet above ground level (agl), temperature -8° C, dew point
-9° C, and altimeter setting 30.12 inches of mercury (Hg). At 0424:57, the captain contacted
company flight operations on the radio to advise that the flight was about 15 minutes out.
At 0433:13, the controller cleared the flight for the ILS approach to runway 17R, and at
0433:52, he instructed the flight to contact the LBB tower. The captain established contact with
the tower, and, at 0434:06, the tower controller cleared the flight to land and reported that the
wind was from 010° at 8 kts.
9
During postaccident interviews, both the captain and the first officer stated that the
airplane accumulated ice during the descent. At 0434:24, the first officer called for a flap setting
of 15°, the deployment of the landing gear, and the landing check. During a postaccident
interview, the first officer recalled that the airplane subsequently accelerated in the descent,
which she stated was unusual for the airplane in a flaps- and gear-down configuration. A
postaccident review of information from the airplane’s flight data recorder (FDR) showed that,
after the first officer called for flaps, the airplane’s airspeed remained about 158 kts and briefly
increased to about 160 kts, and the first officer decreased engine power to about 3 percent torque.
At 0435:03, about the time that the first officer reduced engine power, she stated, “what the heck
is going on?” At 0435:04, the captain replied, “you know what? we have no flaps.”
The FDR showed that a flap asymmetry had occurred in which the right flaps did not
extend and the left flaps extended partially (8° to 10°).
10
The autopilot countered the flap
asymmetry by applying aileron deflection that resulted in a 20° left control-wheel movement.
The FDR indicated that, at the time the captain stated that they had “no flaps,” the airplane was
at an altitude of about 1,400 feet agl just outside the locator outer marker (LOM), which serves
as the final approach fix (FAF).
According to the CVR transcript, after the captain commented about the flap problem,
neither crewmember discussed a procedure or checklist to address it. During a postaccident
interview, the first officer stated that she continued to fly the approach with the airplane coupled
to the autopilot while the captain got out a flashlight and tried to troubleshoot the flap problem.
7
The published procedure specified that the initial climb to 3,700 feet msl is followed by a climbing “left” turn
to “5,000 [feet msl]” via the radial to the intersection.
8
The use of excess vowels, letters, or drawn-out syllables in any word in the CVR transcript is intended to
provide a phonetic representation of the word as spoken.
9
According to the ATR 42 Airplane Flight Manual, the maximum allowable tailwind component for landing is
15 kts. The wind recorded about 0430 by the LBB automated surface observing system was from 360° at 14 kts
gusting to 19 kts.
10
All references in this section to airplane configuration, airspeed, altitude agl, and engine power settings are
derived from the airplane performance study. For more information about the study, see section 1.16.1.

NTSB Aircraft Accident Report
3
The captain stated in a postaccident interview that he repositioned the flap handle several times
and used the flashlight to check the circuit breakers behind the first officer’s seat. The captain
stated that, after finding that no circuit breakers were out, he moved the flap handle back to the
“up” (or 0°) position because he did not want the flaps to travel inadvertently during the
approach.
The FDR indicated that, between 0434:58 and 0435:25, as the airplane descended with
the autopilot engaged, its airspeed decreased from about 160 to 125 kts. At 0435:30 (about
26 seconds after the captain commented about the flap anomaly), the CVR captured a sound
consistent with the aural stall warning (“cricket”) and the tactile stick shaker that lasted
1.1 second. The captain stated to the first officer, “yeah don’t do that.” At 0435:32, a 0.3-second
sound consistent with the aural stall warning sounded. At 0435:36, the captain stated, “just keep
flying the airplane. okay.” The FDR indicated that the stick-shaker activation disconnected the
autopilot when the airplane was about 900 feet agl at 125 kts indicated airspeed (KIAS).
11
The
FDR also indicated that the first officer increased engine power to about 70 percent torque and
began manually flying the approach. Following the application of power, the airspeed began
increasing. At 0435:40, the first officer asked, “should I go around,” and the captain replied,
“no,” and then stated, “keep descending.”
At 0435:44, the first officer stated, “we’re getting close here”; the CVR transcript
indicated that the first officer’s voice sounded as if she were straining. During a postaccident
interview, the captain stated that he looked over and was surprised to see that the first officer was
manually flying the approach and that he had not heard the aural alert to indicate that the
autopilot had been disconnected (no alert was captured by the CVR). The captain asked the first
officer if she wanted him to finish the approach; the first officer replied, “yes please.”
At 0435:50, the captain took control as the PF when the airplane was about 700 feet agl at
143 KIAS. During a postaccident interview, the captain stated that the airplane was high and to
the right of the approach course and that he corrected to put it back on course. According to the
FDR, at 0435:56, the captain reduced the engine power to about 10 percent torque. At 0436:00,
the CVR captured a 0.9-second sound consistent with the aural stall warning and the stick shaker
concurrent with the terrain awareness and warning system (TAWS) warning, “pull up. pull up.”
According to the FDR, at this time, the airplane was about 500 feet agl at 156 KIAS. At 0436:04,
the first officer stated, “there’s the runway.”
Between 0436:00 and 0436:17, as the airplane continued to descend, its airspeed
decreased from about 156 to 129 kts. At 0436:17, the captain called for maximum propeller
speed. At 0436:19, when the airplane was about 200 feet agl at 124 KIAS, the CVR captured the
sounds of engine power increasing concurrent with the aural stall warning and the stick shaker.
At 0436:21, the airplane was about 150 feet agl at 123 KIAS and began to roll right-wing-down
(RWD).
Between 0436:21 and 0436:23, the airplane rolled right to a bank angle of 35° RWD. The
airplane then rolled left to a bank angle of 50° left-wing-down (LWD) bank, and then right
11
The published minimum airspeed for the airplane flying with the flaps retracted in icing conditions was
143 KIAS.
NTSB Aircraft Accident Report
4
reaching a 10° RWD bank before it impacted the ground. At 0436:27, the CVR captured the
sound of impact. During a postaccident interview, the captain reported that he had no lateral
control of the airplane and that the controls were almost “snatched” out of his hands.
An airport operations agent in a vehicle on taxiway M, which parallels runway 17R/35L,
was about 1,800 feet south of the approach end of runway 17R when he saw the airplane
approach. He estimated that the airplane was about 400 to 500 feet agl when it emerged from the
fog layer and stated that it appeared to be high and to the right of the runway centerline. He
stated that the airplane appeared to be “pancaking” in its descent and that it rolled slightly to the
right, then rolled hard to the left in a near-90° bank, then rolled back to the right, impacted the
ground, and slid for a distance. He further stated that, as the airplane slid past his position, a fire
erupted on the airplane’s right wing and “engulfed” the airplane. He stated that he immediately
notified his supervisor of the accident and that he could hear the beeping tones of the crash
phone over his radio as the airplane continued to slide. He stated that he soon saw the lights of
the aircraft rescue and firefighting (ARFF) units emerging from their station.
The airplane came to rest next to the right side of the runway (about 200 feet west of the
runway centerline), north of taxiway S. Figure 1 is an aerial view of the approach end of
runway 17R and the location of the wreckage. The ARFF units, which were on the accident
scene within about 4 minutes, were the first responders to arrive. The ARFF response was joined
by Lubbock Fire Department units, one of which could not enter at the designated airport access
gate because the gate would not open; the unit was diverted to a different gate to enter the
airport.
12
12
For more information about the emergency response, see section 1.15.2.
NTSB Aircraft Accident Report
Figure 1. Aerial view of approach end of runway 17R and location of wreckage.
1.2 Injuries to Persons
Table. Injury Chart
Injuries Flight Crew Cabin Crew Passengers Other Total
Fatal
0 0 0 0 0
Serious
1 0 0 0 1
Minor
1 0 0 0 1
None
0 0 0 0 0
Total
2 0 0 0 2
1.3 Damage to Airplane
The airplane was substantially damaged by the impact forces and postcrash fire.
1.4 Other Damage
The airport approach lighting system and the runway were damaged during the accident
sequence.
5

NTSB Aircraft Accident Report
1.5 Personnel Information
1.5.1 The Captain
The captain, age 52, held an airline transport pilot certificate with ratings for
single-engine and multiengine land airplanes. His most recent Federal Aviation Administration
(FAA) first-class medical certificate was issued on September 19, 2008, with a limitation that he
must “possess glasses for near/intermediate vision.” According to Empire Airlines’ records, the
captain had accumulated 13,935 total flight hours, including 12,742 hours as pilot-in-command
(PIC). He had a total time in the ATR 42 of 2,052 hours, 1,896 hours of which were as PIC. In
the 90 days, 30 days, and 24 hours before the accident, the captain accumulated about 53, 13, and
5 hours, respectively.
The captain was hired by Empire Airlines on May 9, 1988. Employee training records
showed that the captain had previously flown and served as a check airman on the company’s
Cessna 208 (single-engine, turbopropeller-powered) airplanes, in which he had accumulated
about 6,600 total flight hours. He had also previously flown the company’s Fokker F27
(multiengine, turbopropeller-powered) airplanes, in which he had accumulated about 2,500 total
flight hours, about 1,900 hours of which were as PIC. Employee training records showed that the
captain completed his most recent recurrent proficiency check ride and line check on
September 22, 2008. His most recent recurrent ground training, which focused on ATR 42
systems, was completed on March 29, 2008. A review of FAA and company records revealed
that the captain had no previous FAA enforcement actions, incidents, or accidents.
The captain was experienced with in-flight icing conditions because he had worked as a
pilot in the Pacific Northwest and Alaska for 30 years. He stated that he had been dispatched into
freezing drizzle before and that, while flying in such conditions, he maintained a heightened
awareness of the flying environment.
The first officer described the captain as someone whom she would feel comfortable
speaking up to, if necessary. She stated that the captain sought her input and asked for her
opinion and that, at the beginning of their trip pairing, the captain told her that she should tell
him if she saw him do anything wrong. Other Empire Airlines’ pilots who had flown with the
captain stated that his greatest strength as a pilot was his experience level. One pilot stated that
the captain occasionally cut corners, seemed rushed, was less thorough on briefings than other
captains, and became easily agitated when flying and driving.
1.5.2 The First Officer
The first officer, age 26, held a commercial pilot certificate with ratings for single-engine
and multiengine land and instrument airplanes. Her most recent FAA first-class medical
certificate was issued on December 4, 2008, with no limitations. According to Empire Airlines’
records, the first officer had accumulated 2,109 total flight hours, about 1,890 hours of which
were as PIC. She had accumulated 130 hours in the ATR 42 as second-in-command (SIC). In the
90 days, 30 days, and 24 hours before the accident, the first officer accumulated about 88, 29,
and 5 hours, respectively.
6

NTSB Aircraft Accident Report
The first officer was hired by Empire Airlines on July 25, 2008. Employee training
records showed that the first officer completed her most recent proficiency check ride (an initial
check) on September 10, 2008. Her most recent ground training, which was initial training for
the ATR 42, was completed on August 29, 2008. A review of FAA and company records
revealed that the first officer had no previous FAA enforcement actions, incidents, or accidents.
The first officer had limited experience flying in icing conditions before working for
Empire Airlines, and the ATR 42 was the first airplane in which she had flown that was equipped
with deicing and anti-icing systems.
Other Empire Airlines pilots who had flown with the first officer described her flying
skills as “at par” or “average” compared to other first officers with the same experience level.
One pilot stated that the first officer was methodical about using checklists. Another pilot stated
that the first officer’s greatest strength as a pilot was that she was “nonconfrontational.” One
captain described the first officer’s crew resource management (CRM) skills as “good,” and
another captain stated that the first officer did not seem to have a problem speaking up, if
needed. Regarding areas in which the first officer could improve, one pilot stated that “she could
employ the skills she already knew without asking so many questions,” and another pilot stated,
“more hands-on flying of the airplane.”
1.5.3 Flight Crew’s Rest Opportunities
1.5.3.1 The Captain
The captain reported that, on January 24, 2009, he awoke about 0800. From about 1015
to 1535, he traveled as a passenger on commercial flights to reposition from his home in
Portland, Oregon, to Midland International Airport (MAF), Midland, Texas. The captain went to
bed about 2200 in his hotel room in Midland, Texas. On January 25, 2009, the captain awoke
about 0800, performed various activities throughout the day (including exercising, reading,
shopping, and going to dinner at a coworker’s home with the first officer), and went to bed about
2200.
The captain stated that, on January 26, 2009, he awoke about 0400 to prepare for the
upcoming night flight. He performed various activities and then slept from about 1100 to 1630.
He stated that he met the first officer in the hotel lobby about 1820 and that they drove to MAF
to begin duty about 1845. They departed MAF about 1945, arriving at El Paso International
Airport (ELP), El Paso, Texas, about 2115. They subsequently departed ELP for AFW about
2230, arriving about 0030 on January 27, 2009. The flight crew then departed AFW for LBB (the
accident flight) about 0313.
During postaccident interviews, the captain indicated that he needed 6 to 8 hours of sleep
per night to feel rested. He stated that he considered himself to be a night person and that he felt
rested before the accident flight. He described his workload on the day of the accident as normal
overall but stated that, during the approach, the workload was high. The captain stated that
takeoffs and landings were high-workload situations and that the icing conditions and flap
anomaly elevated his workload.
7

NTSB Aircraft Accident Report
8
1.5.3.2 The First Officer
The first officer (who was based in Salt Lake City, Utah)
13
had first arrived in Midland,
Texas, on January 18, 2009, to fly a trip sequence with another captain and had completed that
trip sequence on January 23, 2009. During those trips, the first officer was on duty during night
hours beginning about 0045. After the first officer completed that trip sequence, Empire Airlines
paid the expenses for the first officer to spend the weekend in Midland, Texas, rather than have
her commute home on a short turnaround. The first officer indicated that she was off duty from
the afternoon of January 24, 2009, until the evening of the accident flight. The first officer
indicated that, because her previous trip sequence and the accident trip sequence required her to
sleep during the day and be awake at night, she maintained that same sleep schedule during her
off-duty time (between the two trip sequences) in Midland, Texas.
On January 24, 2009, the first officer went to bed about 0600 in her hotel room and
awoke about 1430. She then performed various activities throughout the day and evening
(including exercising and going to the store) and went to bed about 0600 on January 25, 2009.
She awoke about 1400, later met the captain to go to dinner at a coworker’s home, returned to
the hotel about 2200, and went to bed sometime in the morning on January 26, 2009. The first
officer awoke about 1500 and reported for her trip duty with the captain about 1845.
During postaccident interviews, the first officer indicated that she needed 7 hours of sleep
to feel rested. She stated that she considered herself to be a night person and that she felt rested
before the accident flight. She described her workload on the day of the accident as normal but
stated that the workload became high when she and the captain realized that the flaps did not
function properly. The first officer stated that although the workload during the approach was
high, she felt that it was something that they could handle.
1.6 Airplane Information
1.6.1 General
The accident airplane (model ATR 42-320, serial number [SN] 175) received its
airworthiness certificate in 1990. In 2005, the airplane was configured for freight operations in
accordance with supplemental type certificate (STC) ST01189W1.
14
The airplane was powered
by two Pratt & Whitney Canada PW 121 engines, each equipped with a Hamilton Standard 14SF
propeller. According to the type certificate data sheet, the ATR 42 is certificated for flight in
known icing conditions in accordance with 14 CFR Part 25, Appendix C, which details the types
of icing exposures for which the aircraft is tested and certificated. The airplane’s most recent
inspection (a 2-month inspection) was completed on January 9, 2009. At the time of the accident,
the airplane had accumulated 28,768 hours of operating time and 32,379 cycles.
13
Salt Lake City, Utah, was a “floater” base for Empire Airlines. Flight crews based there would commute to
various cities based on the company’s needs and at the company’s expense.
14
STC ST01189W1 is held by M7 Aerospace LP.
NTSB Aircraft Accident Report
9
The airplane had no deferred maintenance items, and the maintenance records showed
compliance with all applicable airworthiness directives (ADs) for the airframe, propeller
subassemblies, and the right engine.
15
The AD tracking form for the left engine was not located.
During the investigation, an Empire Airlines records clerk located work orders and records of
other required directives to demonstrate AD compliance for the left engine.
The airplane’s maximum gross takeoff and landing weights were 37,258 and
36,155 pounds (lbs), respectively. A review of the FedEx Feeder Aircraft Load Control Sheet
and the Empire Airlines Cargo Load Manifest for the flight revealed that the accident flight’s
calculated takeoff and estimated landing weights were 34,487 and 32,717 lbs, respectively, and
that its calculated center of gravity (CG) was within limits.
1.6.2 Flap System
The ATR 42 is equipped with four trailing-edge flaps (two per wing) that are electrically
controlled and hydraulically operated (each flap has a hydraulic actuator). The flight crew can
command the flaps into four positions using the cockpit flap control lever: 0° for cruise flight,
15° for takeoff and approach, 30° for landing, and 45° for use during an emergency.
16
During
normal operations, all flaps move together when commanded.
An interconnection torque shaft is connected to the left and right inboard flaps. Both a
flap position transmitter, which provides flap position information to the flap indicator in the
cockpit, and a flap asymmetry detector are attached to the interconnection torque shaft. The flap
position transmitter is mounted near the center of the interconnection torque shaft and senses the
average position of the flaps based on movement of the torque shaft. The flap asymmetry
detector is designed to prevent any asymmetry between the right and left flaps from exceeding 8°
to 10° (the precise value depends upon the flap positions when the asymmetry occurs). If a flap
asymmetry reaches the determined value, a microswitch integrated into the detector cuts off the
electrical power supply to the flap control switch, and the flap extension or retraction solenoid is
no longer energized. As a result, the flaps will stop in the positions reached at the time of the
power interruption. Once this occurs, the flaps will not move in response to movement of the flap
control lever in the cockpit until maintenance personnel reset the system on the ground.
17
If a flap asymmetry occurs due to a restriction (jam) and the restriction is then removed,
hydraulic pressure in the system will move the flaps to a symmetrical position. The resulting flap
position will be the average of the right and left flap positions when the asymmetry occurred.
Even if such hydraulic balancing of the flaps occurs, post-flight maintenance action would still
be required to restore electrical power to the flap control switch.
15
The airframe AD compliance records were located throughout the airplane’s records, the propeller
subassembly ADs were tracked through Empire Airlines’ computerized maintenance tracking system, and the right
engine ADs were listed on an AD tracking form located with the right engine logbooks.
16
The four flap positions are standard increments. In the ATR 42, for some selected settings, the actual position
of the flaps differs by a few degrees from the indicator increment (the 30° flap position increment represents 27° of
actual flap deflection).
17
For more information about the flight crew’s procedures for responding to a flap asymmetry, see
section 1.17.1.1.

NTSB Aircraft Accident Report
A flap position indicator in the cockpit has an index marked with the four flap positions
(shown as 0°, 15°, 30°, and 45°), and a needle pointer indicates the flap position on the index. If
a flap asymmetry occurs, the flap indicator needle in the cockpit will point to the index value that
corresponds with the average position of the flaps. Figure 2 shows the flap position indicator,
and the inset depicts the likely needle pointer position during the flap asymmetry.
Figure 2. Flap position indicator. Inset shows the likely needle pointer position during the flap
asymmetry.
In addition to the cockpit flap position indicator, exterior flap position fairings mounted
on the wings (one per wing) are visible to each flight crewmember through their respective side
windows. These fairings are also marked with lines and numbers for the four flap positions,
providing flight crews with a visual indication of the actual position of each flap. Figure 3 shows
the exterior flap position fairing. The wing flap position fairings are illuminated by the wing
lights during nighttime use. If a flap asymmetry occurs, the actual positions of the right and left
flaps will be indicated on the respective flap position fairings.
Figure 3. Exterior flap position fairing.
10

NTSB Aircraft Accident Report
11
1.6.3 Deicing, Anti-Icing, and Anti-Icing Advisory Systems
The ATR 42’s ice protection system permits the airplane to operate in some atmospheric
icing conditions (applicable restrictions are noted in the limitations section of the airplane flight
manual [AFM]).
18
The leading edges of the ATR 42’s wings, horizontal stabilizers, and vertical
stabilizer are equipped with pneumatic deice boots that are inflated by engine compressor bleed
air.
19
When the flight crew selects airframe pneumatic boot use, pockets in the boot system
inflate in sequence, perpendicular to the airfoil, to deice the leading edges.
The propeller blades, windshields, probes (pitot, static, air temperature, and
angle-of-attack [AOA]), and flight control horns
20
are electrically heated. The horn anti-icing
feature prevents ice deposits from forming between the wing structure and the moving parts of
the control surfaces. A pneumatic system provides deicing protection for the engine intakes and
is designed to prevent a reduction or total loss of engine performance in icing conditions.
According to the ATR 42 flight crew operating manual (FCOM), the ATR 42 has an
anti-icing advisory system (AAS) designed to alert the flight crew to apply the correct
procedures when flying in icing conditions.
21
The AAS includes an ice detector (mounted under
the left wing) and three cockpit light annunciators; the amber ICING light and green ICING
AOA light are on the central panel, and the blue DEICING light is on the memo panel. The AAS
alerts the flight crew as soon as (and as long as) the ice detector detects ice accretion. Once the
probe detects at least 0.5 millimeter of ice, the amber ICING light illuminates. The AAS
self-tests continuously, and any failure illuminates a FAULT light with a single chime.
1.6.4 Flight Instruments
1.6.4.1 Airspeed Indicator
The ATR 42 is equipped with three analog airspeed indicators (one on each pilot’s
instrument panel and one on the central panel). Each airspeed indicator has a moving needle
pointer that indicates the airplane’s KIAS on a fixed scale that shows 60 to 400 kts. Each
airspeed indicator has four moveable indices, known as “bugs” (one internal and three external),
on the outer scale that the pilot uses to manually set certain airspeed references for takeoff or
landing, based on airplane performance information for the flight conditions.
22
The internal bug, which is underneath the glass face of the airspeed indicator, is set by the
pilot using a selector knob. According to the ATR 42 pilot handbook, for approach and landing
in icing conditions, the internal bug should be set to V
mHB
30 icing, which is the minimum
18
For more information about these restrictions, see section 1.17.1.6.
19
The vertical stabilizer deice boots are optional on ATR 42s.
20
The airplane’s primary flight controls (ailerons, elevators, and rudder) are mechanically operated and have
counterweights, or horns, that serve to balance the controls.
21
For information about flight crew procedures for responding to each AAS annunciator, see section 1.17.1.6.
22
For information about obtaining applicable airspeed references and setting the bugs, see section 1.17.1.4.

NTSB Aircraft Accident Report
12
approach airspeed and target touchdown airspeed with 30° flaps in icing conditions.
23
The
airspeed indicated by the internal bug (as selected by the pilot using the selector knob) controls
the reference on the electronic attitude direction indicator (EADI) fast/slow scale.
24
The other three indices, which are located on the outside of the glass face of the airspeed
indicator, are color coded for use in referencing certain airspeeds during takeoff or landing and
are manually positioned by the pilot. Unlike the internal bug’s function, the pilot’s positioning of
these three indices (yellow, white, and red) does not affect any other systems or displays. The
ATR 42 pilot handbook states that, for an approach, the yellow bug should be set to reference
V
ga
, which is the approach airspeed for 30° flaps plus 5 kts (not corrected for wind effect).
25
Similarly, the white bug should be set to reference V
mLB
0 normal, which is the minimum
airspeed for an approach with 0° flaps in nonicing conditions, and the red bug should be set to
reference V
mLB
0 icing, which is the minimum airspeed for an approach with 0° flaps in icing
conditions. Figure 4 is an airspeed indicator showing the needle pointer; selector knob; and
internal, yellow, white, and red bugs.
Figure 4. Airspeed indicator showing needle pointer; selector knob; and internal, yellow, white,
and red bugs.
23
The ATR 42 pilot handbook notes that this speed is to be corrected for wind and that the wind factor is 1/3 of
the headwind velocity or the gust in full, with a maximum wind factor of 15 kts.
24
For more information, see section 1.6.4.2.
25
The ATR 42 pilot handbook states that for V
ga
, pilots should use the higher of V
mHB
30 + 5 kts (not corrected
for wind) or 1.1 V
mca
(1.1 times the minimum control airspeed with 5° of bank and the failure of the critical engine
with takeoff flap and landing gear retracted).

NTSB Aircraft Accident Report
13
1.6.4.2 Electronic Flight Information System
The airplane’s electronic flight information system includes displays for each pilot on the
cockpit instrument panel. Each pilot’s display includes an EADI to indicate the airplane’s pitch
and roll relative to the horizon. The EADI depicts the horizon as a straight, horizontal line
between the blue upper half of the display (showing the relative location of the sky), and the
brown lower half (showing the relative location of the ground). The pitch scale is marked in 5°
intervals, and the roll scale indicates select bank angles between 0° and 60°.
The left side of each EADI also displays a “fast/slow” scale that indicates the difference
between the airplane’s actual airspeed and the target airspeed as selected by the pilot using the
internal bug on the airspeed indicator. An index on the fast/slow scale moves up (fast) or down
(slow) according to any deviation of the actual airspeed from the selected airspeed.
1.6.5 Automatic Flight Control System
The airplane was equipped with an automatic flight control system that provided
autopilot, yaw damper, flight director, and altitude alert functions. The autopilot system is
designed to automatically disconnect when certain system conditions occur, including achieving
the stall warning threshold. If an autopilot disconnect occurs (either automatically or manually),
indications provided to the flight crew include an aural alert (“cavalry charge” tone),
26
a message
(“AP DISENGAGED”) on the advisory display unit (ADU), and a visual annunciator (“AP
MSG”) on the primary flight display. With the autopilot system engaged, if an anomaly in the
airplane’s roll characteristics occurs (such as those that a flap asymmetry would induce), the
ADU will show “RETRIM ROLL R [or L] WING DN” and “AILERON MISTRIM” messages.
1.6.6 Stall Protection System
The airplane’s stall protection system includes two AOA probes (one on each side of the
forward fuselage) that detect the airplane’s AOA, an aural stall warning (“cricket”), a tactile stick
shaker, and a stick pusher. According to ATR, when the airplane is configured for flight in
nonicing conditions with flaps 0°, if the AOA probes detect that the airplane has reached a
critical AOA of 11.6°, the aural stall warning sounds, and the stick shaker activates. If the probes
detect that the AOA continues to increase, the stick pusher activates between 11.5° and 13.8°,
depending on the AOA’s rate of change.
The stall protection system is designed to provide an earlier stall warning threshold
during flight in icing conditions. According to ATR, when the airplane is configured with the
control horns’ anti-icing selected on with flaps 0°, the critical AOA for activation of the aural
stall warning and the stick shaker is reduced to 7°, and the stick-pusher activation remains at an
angle between 11.5° and 13.8°.
26
The aural warning can be inhibited by other aural warnings with higher priority.
NTSB Aircraft Accident Report
14
1.7 Meteorological Information
Freezing precipitation in the form of light freezing rain and ice pellets began at LBB
about 2300 on January 26, 2009. The precipitation later changed to light freezing drizzle, which
continued until after the accident.
27
The LBB weather observation about 0353 reported wind from 010° at 14 knots, visibility
3 miles in light freezing drizzle and mist, ceiling overcast at 500 feet agl, temperature -8° C, dew
point -9° C, and an altimeter setting 30.13 inches of Hg. The LBB weather observation about
0453 reported wind from 020° true at 13 kts gusting to 18 kts, visibility 2 miles in light freezing
drizzle and mist, ceiling overcast at 500 feet agl, temperature -8° C, dew point -9° C, and an
altimeter setting 30.13 inches of Hg. The remarks section of the weather observation indicated
that the ceiling was variable from 400 to 900 feet agl and that the hourly liquid equivalent
precipitation was less than 0.01 inch (a trace of precipitation).
The National Weather Service (NWS) terminal aerodrome forecast for LBB expected
IFR conditions to prevail during the period including the accident flight’s arrival with wind from
030° at 12 knots, visibility of 1 1/2 miles in light freezing drizzle and mist, and ceiling overcast
at 100 feet agl through about 0800, with a temporary period of visibility 1/2 mile in light freezing
drizzle and freezing fog. The NWS also had issued an airmen’s meteorological information
(AIRMET) for moderate icing conditions
28
from the freezing level through 22,000 feet msl over
Texas that was current at the time of the accident. A review of the NWS current icing potential
and supercooled large droplet (SLD) icing diagnostic charts indicated a greater-than-80-percent
probability of icing conditions over the LBB area from the surface through 6,000 feet msl and a
high likelihood of encountering SLD conditions. Temperatures were above freezing between
6,000 and 11,000 feet msl as a result of a temperature inversion.
1.8 Aids to Navigation
No problems with any navigational aids were reported.
27
As defined by the American Meteorological Society Glossary and the National Weather Service Federal
Meteorological Handbook, freezing drizzle is drizzle that falls in liquid form but freezes upon impact with surfaces
to form a coating of glaze; freezing drizzle has a diameter between 0.05 to 0.5 millimeters (0.002 to 0.02 inches) at
temperatures less than 0° C.
28
According to the FAA’s Aeronautical Information Manual (AIM), when reporting icing to air traffic control,
pilots should describe the icing intensity as moderate when the rate of accumulation is such that even short
encounters become potentially hazardous and use of deicing/anti-icing equipment or flight diversion is necessary.
Information obtained from the FAA’s website <http://www.faa.gov/air_traffic/publications/ATpubs/AIM/>
(accessed March 21, 2011). FAA Advisory Circular 91-74A, “Pilot Guide: Flight In Icing Conditions” published in
December 2007, states that, in icing of moderate intensity, “the rate of ice accumulation requires frequent cycling of
manual deicing systems to minimize ice accretions on the airframe. A representative accretion rate for reference
purposes is 1 to 3 inches (2.5 to 7.5 cm) per hour on the outer wing. The pilot should consider exiting the condition
as soon as possible.”
NTSB Aircraft Accident Report
15
1.9 Communications
No problems with any communications equipment during the flight were reported.
During a postaccident interview, the first officer stated that, after the accident, the captain
attempted to contact the air traffic control tower (ATCT) using the airplane’s radios but that the
radios were inoperative. The CVR transcript indicates that the CVR captured the sound of impact
at 0436:27, a subsequent sound similar to occupants moving around in the cockpit, the captain’s
instructions about exiting the airplane, and the sound of the door opening at 0437:25. No further
sounds were captured, and the recording ended at 0441:35.
1.10 Airport Information
LBB is located about 4 miles north of the city of Lubbock, Texas, at an elevation of
3,282 feet msl. LBB is a Class I public airport certificated under 14 CFR Part 139.
29
Runway
17R/35L, which is the longest of the airport’s three runways,
30
has a concrete surface and is
11,500 feet long and 150 feet wide.
LBB maintained ARFF capabilities at Index C
31
and had four vehicles, three of which
(Rescue 1, 2, and 4) were equipped with a roof turret, bumper turret, and hand line; each vehicle
carried 1,500 gallons of water, at least 190 gallons of aqueous film forming foam (AFFF), and
450 lbs of dry chemical. The remaining vehicle (Rescue 5), which was equipped with a hand
line, carried 450 lbs of dry chemical and 100 gallons of a mixture of water and AFFF. The ARFF
station was centrally located south of taxiway J near the midpoint of runway 8/26. ARFF
services were available 24 hours a day, every day, and the station was staffed by a minimum of
four firefighters. Five firefighters, all of whom participated in the response, were on duty at the
time of the accident.
32
1.10.1 Emergency Plan
LBB had an FAA-approved airport emergency plan (AEP) that provided guidance
intended to minimize the possibility and extent of personal injury and property damage during an
emergency. The FAA approved the most recent revisions to the AEP on July 9, 2008. The AEP
stated that, during an emergency response, “primary entry points to the airfield by responding
units will be at Gate 6 and Gate 48 or at a location prescribed by the command post.” The AEP
stated that “the Battalion Chief will set up the initial staging area/command post near Gate 6,
Gate 48, or another designated area.”
29
Title 14 CFR 139.5 states that a Class I airport is certificated to serve scheduled operations of large air carrier
aircraft and can also serve unscheduled passenger operations of large air carrier aircraft and/or scheduled operations
of small air carrier aircraft.
30
Runway 8/26, which has a concrete surface, is 8,001 feet long and 150 feet wide, and runway 17L/35R,
which has an asphalt surface, is 2,891 feet long and 75 feet wide.
31
LBB was an Index C airport based on five or more average daily departures of aircraft with a length of at
least 126 feet but less than 159 feet, as defined in 14 CFR 139.315. For an airport to meet Index C capabilities,
14 CFR 139.317 requires two or three ARFF vehicles that contain at least the minimum specified amount of various
extinguishing agents.
32
For more information about the emergency response, see section 1.15.2.

NTSB Aircraft Accident Report
16
If an accident occurs, the ATCT notifies the ARFF station through the direct line radio to
the station. According to the letter of agreement between the LBB ATCT and the City of
Lubbock, upon the alert activation, the ATCT controller should provide, “as is available,” the
“type of aircraft, nature of the emergency, runway to be used, and any other information if time
permits.”
1.10.2 Snow and Ice Control Plan
As required by 14 CFR 139.313, LBB maintained an FAA-approved snow and ice
control plan. According to the airport’s snow and ice operations document, the operations
supervisor, operations agent on duty, or maintenance supervisor is responsible for monitoring the
runway and taxiway environment to determine when snow and ice removal is needed. Sensors
embedded at various points on the runways, taxiways, and the terminal ramp detect surface and
subpavement temperatures and surface moisture, and information from the sensors is monitored
from the airfield maintenance building by airport maintenance personnel.
The snow and ice operations document indicated that, during critical temperatures, if
moisture or precipitation is occurring or is expected to occur, granulated urea will be applied to
the first priority airport operational surfaces, such as the active runway, its parallel taxiway,
taxiways connecting the active runway to the terminal ramp, and the established ARFF road
from the fire station to taxiway J. The assistant airport manager stated that the road from the fire
station to taxiway J had received a urea application before the accident flight’s arrival. No
written record exists to indicate when this application occurred.
The snow and ice operations plan did not address monitoring or ensuring the operability
of the airport emergency response and mutual aid gates. FAA Advisory Circular (AC)
150/5200-30C, “Airport Winter Safety and Operations,” which provides guidance to assist
airport operators in developing a snow and ice control plan, also did not address this topic. An
informal survey of other 14 CFR Part 139 airports where operations are affected by winter
weather revealed that none of the airports’ snow and ice control plans addressed gate operability.
1.11 Flight Recorders
1.11.1 Cockpit Voice Recorder
The accident airplane was equipped with a Fairchild Model A100A CVR, SN 59653,
capable of recording four channels of analog audio on a continuous loop tape. An examination of
the CVR at the National Transportation Safety Board’s (NTSB) vehicle recorders laboratory
found no evidence of structural or heat damage, and audio information was extracted without
difficulty.
The extracted 30-minute, 43-second recording consisted of three channels of useable
audio information that captured events from before the flight’s descent to several minutes after
the accident. Excellent quality audio
33
was obtained from the channels for the captain’s and the
33
In an excellent quality recording, virtually all of the crew conversations can be accurately and easily
understood, and only one or two words are not intelligible; any loss is usually attributed to simultaneous cockpit

NTSB Aircraft Accident Report
17
first officer’s audio panels, and good quality audio was obtained from the channel for the cockpit
area microphone. The fourth channel (the use of which was not required by Federal regulations)
contained no audio information.
1.11.2 Flight Data Recorder
The accident airplane was equipped with a Fairchild Model FA2100 FDR, SN 289112.
The FDR was sent to the NTSB’s laboratory for readout and evaluation; it was received in good
condition, and the data were extracted normally from the recorder. The FDR recorded about
56 hours of data, and the accident flight is reflected in the final 2 hours 18 minutes of the
recording. The FDR system was configured to record more than 70 parameters of airplane flight
information in a digital format using solid-state flash memory as the recording medium. For this
investigation, 58 parameters that were considered relevant were verified and examined. The
relevant parameters included flap position, flap asymmetry, left and right aileron surface
positions, KIAS, glideslope and localizer deviations, radio altitude (altitude as sensed by the
radio altimeter), AOA, roll, pitch, pitch trim, right control column position, control wheel
position, airframe deicing, left and right elevator positions, and left and right engine propeller
speed.
34
1.12 Wreckage and Impact Information
Examination of the accident site showed that the airplane initially impacted flat, grassy
terrain about 300 feet north of the runway 17R blast pad.
35
Ground scars and debris from the
airplane extended about 2,500 feet south from that location to where the main wreckage came to
rest next to the right side of the runway (about 200 feet west of the runway centerline), north of
taxiway S. Fragments of the nose landing gear, right main landing gear, and a separated outboard
section of the right aileron were identified in the initial debris field near the beginning of the
runway.
Examination of the wreckage found that the airplane was resting on its nose section and
leaning to the right; the left main landing gear remained attached. Sections of the upper fuselage,
right wing, and right inboard and outboard flaps were destroyed by fire. The left engine remained
secured to the wing, and the left propeller sustained minimal damage. The right engine and the
right propeller sustained impact and fire damage.
conversations and/or radio transmissions that obscure each other. In a good quality recording, most of the crew
conversations can be accurately and easily understood, but several words or phrases are not intelligible; any loss can
be attributed to minor technical deficiencies, momentary dropouts in the recording system, or a large number of
simultaneous cockpit conversations and/or radio transmissions that obscure each other.
34
For information regarding the relevant parameters that were used in performing the airplane performance
study, see section 1.16.1.
35
A blast pad, which is unusable for landing, takeoff, or taxiing, is designed to eliminate the erosive effect of
the high wind forces produced by airplanes at the beginning of their takeoff roll. The blast pad for runway 17R is a
concrete extension north of the threshold that can also serve as a stopway in the event of a rejected takeoff on
runway 35L.

NTSB Aircraft Accident Report
18
1.13 Medical and Pathological Information
On the morning of January 27, 2009, the captain and the first officer participated in
breath analysis testing for alcohol and provided urine specimens for company drug testing.
36
The
tests yielded no evidence of alcohol or drug use by either crewmember.
1.14 Fire
A fuel-fed fire erupted during the accident sequence and destroyed sections of the
airplane and some cargo before being suppressed by firefighting personnel. According to the
airplane’s dangerous goods manifest, 25 lbs of dry ice, one package of seatbelt pretensioners,
and two containers of materials classified as “ORM-D [other regulated materials-domestic]
consumer commodity” were destroyed in the fire. Other hazardous material (HAZMAT) on
board, which included five containers of liquid chloride, one container of liquid sodium chlorite,
and one container of solid sodium iodine (all radioactive materials), were undamaged.
1.15 Survival Aspects
1.15.1 Flight Crew Egress
According to the CVR transcript, after the airplane came to a stop, the captain told the
first officer to “go out the hatch” but then stated, “there’s a fire on the right hand side. go out the
left.” During a postaccident interview, the first officer stated that she first opened the cockpit
escape hatch and saw a “raging fire” on the airplane’s right side. She stated that she then went to
the forward cargo door, unlocked it, and pushed it open with the help of the captain. The first
officer stated that they “jumped out and ran to FedEx.” The captain stated that, once they were
outside the airplane and a safe distance from it, he called Empire Airlines’ dispatch to report the
accident. Both the captain and the first officer left the accident scene before the first responders
arrived.
1.15.2 Emergency Response
The ATCT notified the ARFF station of the accident through the direct line radio.
According to LBB ARFF personnel, a tone sounded in the fire station, followed by “muffled
voices.” Shortly thereafter, a second tone sounded, and an Alert 3 (which indicates an accident
on or near the airport) was announced. According to the dispatch logs from the Lubbock Fire
Department, the alarm sounded at 0438:12, and three ARFF units (Rescue 2, 4, and 5) were
dispatched at 0438:46 and arrived on scene at 0442:31.
The ARFF captain, who was driving Rescue 5, reported that the three ARFF units
proceeded along taxiway J toward taxiway M. He stated that ice was on the runways and taxiway
and that he proceeded with caution because of the potential for slippery conditions. The ARFF
equipment operator driving Rescue 2, which also carried an ARFF lieutenant and another
36
Empire Airlines’ drug testing program checked the samples provided for evidence of marijuana, cocaine,
amphetamines, opiates, and phencyclidine use.
NTSB Aircraft Accident Report
firefighter, estimated that they proceeded no faster than 45 mph. While en route to the accident
site, the ARFF equipment operator driving Rescue 2 contacted the ATCT controller to ask what
type of airplane had crashed and how many passengers were on board; the ATCT controller
replied that it was an ATR carrying an unknown number of people.
The ARFF lieutenant in Rescue 2 stated that the darkness and fog made it difficult at
times to distinguish between smoke and fog. The ARFF captain driving Rescue 5 stated that,
after turning onto taxiway M, he saw both smoke and the glow from the fire. The ARFF captain
stated that heavy smoke and flames engulfed the airplane from the cockpit to the wing section
and extended just aft of the wing, where most of the flames were present. The ARFF equipment
operator driving Rescue 2 stated that they immediately began applying foam and water to the
wreckage and, within about 45 seconds, suppressed the fire to the extent that they could see the
FedEx logo on the airplane’s tail. He indicated that, because of the logo, he knew that it was a
cargo airplane and that he would expect two to three occupants. He stated that he then heard
Rescue 5’s call to start looking for survivors.
The ARFF captain stated that the fire was “blackened down” quickly. The ARFF
lieutenant from Rescue 2 accessed the cabin area from a burn hole in the fuselage to look for
occupants, and another firefighter from Rescue 2 used a ladder to access the cockpit roof hatch to
look inside. After observing that no one was inside the airplane, ARFF personnel from Rescue 2
and Rescue 5 immediately began searching the area for the airplane’s occupants by performing
visual and thermal imaging searches.
According to standard protocol for an Alert 3 accident, Lubbock Fire Department units
also responded and were dispatched at 0441:10. The response included the battalion chief and
engine from Station 2 (which is about 3.2 miles from LBB and staffed with personnel who are all
ARFF-certified firefighters with airport access badges); an engine from Station 5 (about 7 miles
from LBB); and an engine, truck, and HAZMAT team from Station 4 (about 7 miles from LBB).
As directed, one engine from Station 2 responded to Gate 48, which is an electronically
controlled gate operated by a drive chain. The engine team was unable to enter the airport
property at Gate 48 because the gate had ice in its operating mechanism and would not open. The
Station 2 engine then drove to the ARFF station to proceed from that point. All other responding
Lubbock Fire Department units were informed that the wreckage was closest to the FedEx
hangar and were rerouted to respond to that site. A FedEx employee who opened the gate near
the FedEx hangar for the Station 2 team, Station 5 engine, and emergency medical service
(EMS) personnel informed them that the pilots were at the hangar; the EMS units proceeded to
the hangar. Figure 5 is a view of the airport showing the relative locations of airport access gates
and the accident site.
19

NTSB Aircraft Accident Report
Figure 5. View of airport showing relative locations of airport access gates and accident site.
The first Lubbock Fire Department unit arrived on scene at 0457:27. At that time, the
ARFF units had contained the fire, with the exception of a few deep-seated cargo fires inside the
airplane. The Lubbock Station 2 battalion chief assumed incident command and informed the
ARFF captain that the flight crew was at the FedEx hangar. The ARFF captain stopped the
search for survivors, and ARFF personnel resumed their fire suppression activities. The Station 2
battalion chief and ARFF personnel indicated that the ATCT controller later called and stated
that a pilot was walking around on the ramp looking for assistance, and a second search for
survivors was initiated. ARFF personnel determined that both pilots were being transported to a
local hospital, and the emphasis on fire suppression resumed.
The Lubbock battalion captain (who assumed command of operations from the Lubbock
Station 2 battalion chief) stated that, about 5 to 10 minutes after he arrived on scene, the
Lubbock Police Department delivered a HAZMAT manifest that FedEx employees had
provided. The fire department had not requested the information. The Lubbock Station 2
battalion chief stated that the HAZMAT team responded to the FedEx hangar to obtain the
material safety data sheets for the materials on the HAZMAT manifest. The ARFF captain stated
that he did not see the HAZMAT manifest on the airplane but that he was aware that such a
document existed and was available. The ARFF captain stated that the ARFF response to the
accident scene would have been similar if they had known that HAZMAT was on board the
airplane, with the exception that all responding firefighters would have worn full personal
protective equipment.
20
NTSB Aircraft Accident Report
21
1.16 Tests and Research
1.16.1 Airplane Performance Study and Simulator Evaluations
The NTSB conducted an airplane performance study to estimate the airplane’s position,
airspeed, altitude, and other parameters throughout the accident flight. Data sources for the study
included the airplane’s FDR, FAA air traffic control (ATC) radar data, and weather information
services.
37
The study extracted aerodynamic coefficients from the FDR data. In addition, ATR
used its ATR 42-320 engineering model to which accident flight-specific information was
applied (including FDR data and weather information) to estimate control forces, AOA, and ice
accretion levels during the accident flight. Further, the NTSB used an ATR 42-320 engineering
flight simulator (EFS) provided by ATR to conduct qualitative testing to assess pilot workload
and to evaluate the airplane’s handling qualities with a flap asymmetry and ice accretion. The
EFS could not reproduce the accident airplane’s drag levels from ice accretion without
introducing unrealistic lift and pitch, roll, and yaw moments;
38
as a result, the “Normal Icing—
Boots On” ice levels were used with the knowledge that the drag effect was underestimated.
Pilots from ATR, Empire Airlines, and the NTSB participated in the EFS qualitative testing.
1.16.1.1 Effects of Flap Asymmetry
The flap asymmetry involved 8° to 10° of extension of the left flap and no extension of
the right flap. The greater flap extension on the left wing resulted in more lift and drag on that
wing; as a result, the airplane banked to the right. According to the FDR, the autopilot system
countered the airplane’s right bank by introducing 6° of left aileron input, for which the autopilot
moved the control wheel about 20° to the left.
The FDR indicated that, at 0434:55 (about 30 seconds after the flap asymmetry
occurred), the first officer reduced engine power from about 58 percent torque to about
3 percent. The autopilot, which was coupled to the ILS 17R approach, responded by increasing
the pitch attitude of the airplane to maintain the glideslope for the approach. The airplane’s
airspeed decreased to the point that, at 0435:30, the stick shaker activated, which disconnected
the autopilot when the airplane was about 1,000 feet agl. The performance study showed that the
stick shaker triggered at about an AOA of 7.2°, a load factor of 1.08 G, and an airspeed of
125 kts.
The FDR indicated that, after the autopilot disconnected (and the first officer began to
manually fly the approach), the first officer increased engine power to about 70 percent torque,
and the airplane began to deviate high and to the right of the ILS 17R glidepath.
39
Control force
37
The study results are estimates that include performance calculation assumptions and consider the inherent
limitations of the input data sources.
38
Title 14 CFR Part 60, which contains the qualification performance standards for airplane EFS models,
specifies that the effects of airframe icing (including airspeed decay and change in simulator pitch attitude) can be
based on subjective tests; that is, an EFS’s presentation of these effects is not required to match actual airplane
performance data obtained from airplane icing testing, incidents, or accidents.
39
The glidepath, which is the ideal flightpath for an ILS approach, is formed by the intersection of localizer
plane (which provides horizontal course guidance along the extended runway centerline) and glideslope plane
(which provides vertical course guidance).
NTSB Aircraft Accident Report
22
estimates that ATR provided indicated that the first officer was applying about 35 to 40 lbs of
rudder pedal pressure. ATR estimated that the average control wheel force required to manually
counter the flap asymmetry without retrimming the airplane was about 13 lbs.
At 0435:50, the captain took control of the airplane, and the estimated pilot forces exerted
on the cockpit controls peaked about 10 seconds later when the captain pulled back on the
control column, input LWD control wheel, and pushed on the left rudder pedal. ATR estimated
that the maximum forces exerted on the control column, control wheel, and rudder pedals were
about 36, 29, and 112 lbs, respectively. The FDR indicated that, at the time that these maximum
forces were applied, the airplane was about 500 feet agl and more than 300 feet right of course
(in the cockpit, this position would have displayed as “two dots” right on the course deviation
indicator),
40
and the stick shaker activated again. The performance study showed that the stick
shaker triggered at about an AOA of 6.8°, a load factor of 1.64 G, and an airspeed of 155 kts.
FDR data indicated that, at 0436:02 (about 2 seconds after the captain’s application of
high control forces), the control wheel and the ailerons moved from the deflected positions that
compensated for the flap asymmetry to their nominal positions. This movement was consistent
with the left-wing flaps retracting to approximately 4.5°, and the right-wing flaps extending to
approximately 4.5°, rendering all four wing flap panels symmetric, thus removing the need for
control inputs to counteract the flap asymmetry.
1.16.1.2 Effects of Airframe Ice Accretion
FAA inspectors who observed the wreckage about 3 hours 20 minutes after the accident
noted that the separated outboard section of the right aileron (which was found outside the fire
area) had an 8-inch patch of 1/8-inch thick ice adhered to the underside. The adhered ice patch
had jagged edges, as if some portions of ice had broken away from it. As noted in the
Aeronautical Information Manual (AIM),
41
section 7-1-21, “the effects of ice on aircraft are
cumulative; thrust is reduced, drag increases, lift lessens, and weight increases. The results are an
increase in stall speed and a deterioration of aircraft performance.”
The NTSB’s aerodynamic coefficient extraction and calculations made by ATR indicated
that airframe ice accretion during portions of the flight degraded the airplane’s performance. The
ATR calculations indicated that the airplane first encountered icing at the beginning of cruise
flight at flight level (FL) 180 (18,000 feet pressure altitude). ATR calculated that, at the end of
cruise flight at FL 180, a drag increase corresponding with about 15 percent of total power was
present. The aerodynamic coefficient extraction showed an increment in drag beyond the level
expected for an uncontaminated airframe from about 0335 to 0405 while the aircraft was in
cruise flight.
The ATR calculations indicated that, during the descent between 14,000 to about
5,000 feet msl, the airplane’s performance was consistent with what would be expected for an
40
Course sensitivity at this point in the approach is such that one dot represents about 150 feet of horizontal
course deviation.
41
Information obtained from the FAA’s website <http://www.faa.gov/air_traffic/publications/ATpubs/AIM/>
(accessed March 21, 2011).

NTSB Aircraft Accident Report
23
uncontaminated airframe (free from ice accumulation). The aerodynamic coefficient extraction
showed the drag level expected for an uncontaminated airframe from about 0405 to about 0432.
However, beginning about 0432 when the aircraft was at 5000 feet msl, an increment in drag
beyond the level expected for an uncontaminated airframe was again seen. ATR calculated that,
by the time that the flap asymmetry occurred, a drag increase corresponding with about
23 percent of total power was present. The EFS qualitative testing revealed that, following the
autopilot disconnect, the workload for the accident flight crew was high because of the flap
asymmetry, a 10-kt tailwind, and ice accretion. The testing showed that, when the approach was
continued without retrimming the airplane and at a speed lower than the minimum safe airspeed
of 143 KIAS (conditions similar to the accident flight), the controllability of the simulator was
often similar to what the FDR data showed for the accident airplane. However, when the
“AILERON MISTRIM” checklist in the Empire Airlines’ ATR quick reference handbook
(QRH) was applied
42
and engine power was set to maintain the minimum safe airspeed, the
pilots who conducted the EFS qualitative testing performed a missed approach (go-around
procedure when under IFR), completing the QRH procedures for the flap anomaly and the
reduced-flaps landing, and successfully landing the airplane.
FDR data indicated that, at 0436:18 (about 9 seconds before impact), the captain began a
pull back on the control column that lasted for several seconds. When the pull back began, the
airplane was at an airspeed of about 125 kts, descending through 230 feet agl about 1,500 feet
per minute (fpm); the pitch attitude was about -0.5°, and the load factor was about 0.9 Gs. In
response to the captain’s pull on the control column, the pitch attitude, the AOA, and the load
factor all began to increase. The performance study showed that when the stick shaker triggered
for the third time at 0436:19, the AOA was about 7°, the load factor was about 1.02 G, and the
airspeed was about 124 kts.
At 0436:20 (about 7 seconds before impact), with the AOA and the pitch attitude still
increasing, the load factor stopped increasing about 1.12 Gs, indicating that an aerodynamic stall
was imminent.
1.16.2 Terrain Awareness and Warning System
The airplane was equipped with a TAWS
43
designed to provide terrain caution alerts,
“pull up” warnings, and “avoid terrain” warnings. Data analysis showed that, when the TAWS
provided the flight crew with the aural “pull up” warnings, the airplane was about 1.5 miles from
the runway threshold at an altitude of 488 feet agl (as detected by the radio altimeter) with a
vertical descent rate of 2,050 fpm. An event analysis report provided by Aviation
Communication & Surveillance Systems, the manufacturer of the integrated system with the
TAWS feature, indicated that, during the accident approach, the airplane’s low radio altitude
combined with the rapid change in vertical speed resulted in the immediate TAWS warning
without a preceding caution alert.
42
For information about the procedure, which involves retrimming the airplane and then reengaging the
autopilot, see section 1.17.1.5.
43
This particular TAWS was part of an integrated system that also provided traffic alert and collision avoidance
functions.

NTSB Aircraft Accident Report
1.16.3 Flap System Component Examinations
The cockpit flap control lever was found in the 15° position. Examination of the flap
system components at the accident site found that the left wing and flap components were intact
and covered with soot. The right inboard and outboard flaps and the right inboard flap actuator
were extensively damaged by impact and fire. Figure 6 is the right side of the fuselage, showing
extensive fire damage to the right wing and flap components. The right outboard flap actuator
was found in the retracted position on the ground under the right wing. Damage to the right flaps
limited the extent to which preimpact system integrity could be determined. Examination of the
available components revealed no evidence of mechanical restriction of movement of the right
flaps.
Figure 6. Right side of fuselage showing extensive fire damage to right wing and flap
components.
Under normal circumstances, hydraulic pressure holds the flaps in the selected position.
The accident airplane’s hydraulic system was damaged by impact and fire, and much of the
hydraulic fluid routed to the flap actuators was lost because of the damage. Testing of fluid
samples obtained from all actuators (either from the actuator itself or the line leading to the
actuator) found that the liquid was consistent with hydraulic fluid.
X-ray examinations of all four flap actuators showed that their internal components were
in place. The left inboard and left outboard flap actuators functioned when tested on the test
bench at the manufacturer’s facility. Subsequent disassembly and examination of the left inboard
and outboard flap actuators revealed no anomalies. Several of the seals for the right inboard and
right outboard flap actuators were damaged from fire exposure, and the damage prevented the
24

NTSB Aircraft Accident Report
25
actuators from functioning on the test bench. Disassembly of the right inboard and outboard flap
actuators revealed no evidence of jamming.
Regarding the possibility that ice formation on the flap surfaces could have resulted in a
flap asymmetry, ATR stated that, in all types of icing conditions, runback icing does not exceed
15 to 20 percent of the wing chord on the upper wing surface and 30 to 40 percent of the wing
chord on the lower wing surface and that these limits are upstream of the flaps. Further, ATR
noted that ATR models having a similar wing/flap design have accrued 17,567,000 flight cycles
with no reports of flap asymmetry or jamming due to flight in icing conditions.
1.16.3.1 Hydraulic Fluid Testing
The piston rod for the right outboard flap actuator was found coated with a green material
for which chemical testing was inconclusive. Solid particles, which testing found to be consistent
with heated hydraulic fluid, were found in the hydraulic fluid lines and the connector port for the
right outboard flap actuator. No similar particles were found in any fluid samples from the
airplane’s hydraulic reservoir or from the examined hydraulic system filters.
1.16.3.2 Maintenance History
According to ATR, flap actuators are not subject to time limitations; they are serviced or
replaced based on their condition. At the time of the accident, the right inboard flap actuator and
the left outboard flap actuator were original equipment to the airplane (installed when it was
manufactured). The right outboard flap actuator and the left inboard flap actuator were installed
in February 2001.
Empire Airlines’ maintenance records indicated that a flap actuator hardware inspection
was completed on June 4, 2007. On October 31, 2007, during a takeoff configuration test
performed during taxi, the flaps did not extend but then functioned normally after subsequent
maintenance action to clean deicing fluid from the cannon plug. The airplane had been involved
in a January 21, 1998, accident in which a fuel-fed fire erupted in the right engine bay after
landing, which substantially damaged the airplane and exposed several components on the right
wing, including the flaps, to fire damage.
44
The airplane’s log books showed that the airplane
had been repaired, inspected, and returned to service.
1.16.3.3 Flap Asymmetry Event Involving Another Airplane
According to ATR, one previous flap asymmetry event was reported in 1996 involving an
ATR 42-500. The event occurred during a maintenance positioning flight (the maintenance was
related to a problem with the right powerplant that occurred on the previous day). During the
positioning flight, the asymmetry occurred when the flight crew commanded flap extension. The
airplane landed without incident, and the reason for the flap asymmetry was not determined.
44
The NTSB determined that the probable cause of the accident was “the improper overhaul of lug holes on the
fuel/oil heat exchanger. A factor was the lack of direction contained in the manufacturer’s overhaul manual for
working with the lug holes.” The report for this accident, NTSB case number NYC98FA062, is available online at
<http://www.ntsb.gov/aviationquery/index.aspx>.
NTSB Aircraft Accident Report
26
1.16.4 Deicing and Anti-Icing System Examinations
The pneumatic deicing boots on the left wing and the empennage were tested, and no
preimpact anomalies were identified. Impact and fire damage to the pneumatic boots on the right
wing prevented testing. The distributor valves for the airframe pneumatic boots were tested, and
all of the valves opened and closed as designed. All electrically heated components were
examined, and a resistance was obtained. Examination of the AAS annunciator panel by the
NTSB’s materials laboratory revealed no evidence of filament stretching in any bulbs.
1.16.5 Autopilot Disconnect Alert
The crew alerting computer, flight guidance computer, flight guidance controller, and
ADU were tested after the accident, and the autopilot disconnect and alerting systems functioned
normally. The autopilot disconnect aural alert sounded as designed. According to ATR, the
control wheel is equipped with an autopilot disconnect push button. Pressing the button while the
autopilot is engaged disconnects the autopilot. Pressing the button while the autopilot is
disconnected (whether disconnected manually with the button or by stick-shaker activation)
clears any messages from the ADU and silences any pending autopilot disconnect alert.
1.17 Organizational and Management Information
Empire Airlines, headquartered in Hayden, Idaho, provides cargo operations under
14 CFR Parts 135 and 121. The company, which has evolved under different names and has
provided a variety of services (including some passenger-carrying operations) since 1977,
45
began Part 121 operations in 1989. During that same year, Empire Airlines began a contract with
FedEx for cargo services using Fokker F27 airplanes. The company continued to evolve its fleet
and services and ended all passenger-carrying operations in 1995 to focus on cargo operations,
aircraft maintenance, and airline startups.
46
The company obtained a 14 CFR Part 145 repair
station certificate under the name of Empire Aerospace in 2001. It acquired its first ATR 42
airplane in 2003 and performed its first ATR 42 revenue flight for FedEx in 2004.
At the time of the accident, Empire Airlines had 16 bases of operation and served
51 destinations as a feeder operator for FedEx. According to the managing director of FedEx
feeder operations, FedEx’s relationship with its feeder operators is a fee-basis system in which
45
The company was first established as Clearwater Flying Service in 1977 and, by 1979, operated flights for
fire patrol, air pollution monitoring, air ambulance, charter, flight instruction, and transporting outfitters to remote
areas. In 1980, after acquiring another company, Clearwater Flying Service changed its name to Empire Airways
and expanded its services to include aircraft sales and maintenance. In 1986, the company contracted to operate
shuttle flights between ski resorts, and, in 1987, the company expanded with contracts to fly corporate employees
between offices in California and to perform flights in Alaska for the Naval Arctic Research Laboratory. Later that
same year, Empire Airways contracted with FedEx to fly and maintain Cessna 208 airplanes and to service routes
throughout the Pacific Northwest. In 1989, Empire Airways purchased Pacific Alaska and two Fokker F27 airplanes,
and the company changed its name to Empire Airlines.
46
Empire Airlines added turbojet airplanes for some operations in 1992. The company also assisted a startup
airline in Hawaii in 1992 and assisted another airline in Europe (to provide services for FedEx) in 1998. In 2006, the
company’s operations specifications authorized it to perform heavy maintenance on ATR 72 and Fokker F27
airplanes, and it later obtained heavy maintenance authorizations for de Havilland DHC-8 and Q400-series
airplanes.

NTSB Aircraft Accident Report
the operators are paid a management fee to crew and maintain the airplanes. At the time of the
accident, Empire Airlines operated 10 ATR 42, 3 ATR 72, and 35 Cessna 208 airplanes, all of
which were owned by FedEx. Empire Airlines employed about 250 people, including 108 pilots,
34 to 40 mechanics, and 7 flight followers.
1.17.1 Pilot Standard Operating Procedures and Training
Empire Airlines’ general operations manual (GOM) provided flight crews with
information on the company’s standard operating procedures (SOPs). Flight crew procedures
specific to the airplane were found in the ATR 42 AFM, which was an FAA-approved manual
that contained the normal, abnormal, and emergency procedures. The Empire Airlines ATR 42
QRH listed the procedures in a cockpit checklist format.
Empire Airlines provided its pilots with company indoctrination training at company
headquarters. Empire Airlines’ operations specifications authorized that all other initial,
recurrent, upgrade, and transition ground training, simulator training, testing, and checks were to
be provided by FlightSafety International, Inc., in Houston, Texas.
1.17.1.1 Flap Anomalies
According to the QRH, one procedure covered multiple flap anomaly conditions,
including a jam, uncoupling, or asymmetry. The procedure, “FLAPS
JAM/UNCOUPLED/ASYM,” specified that the pilot should position the flap control lever to
correspond with the actual flap position and apply the “REDUCED FLAPS LANDING”
procedure. Figure 7 is the QRH, page 2.21, with “FLAPS JAM/UNCOUPLED/ASYM” and
“REDUCED FLAPS LANDING” procedures. Pilots are trained to perform a go-around
maneuver in response to a flap anomaly so that they will have time to perform these required
procedures.
27
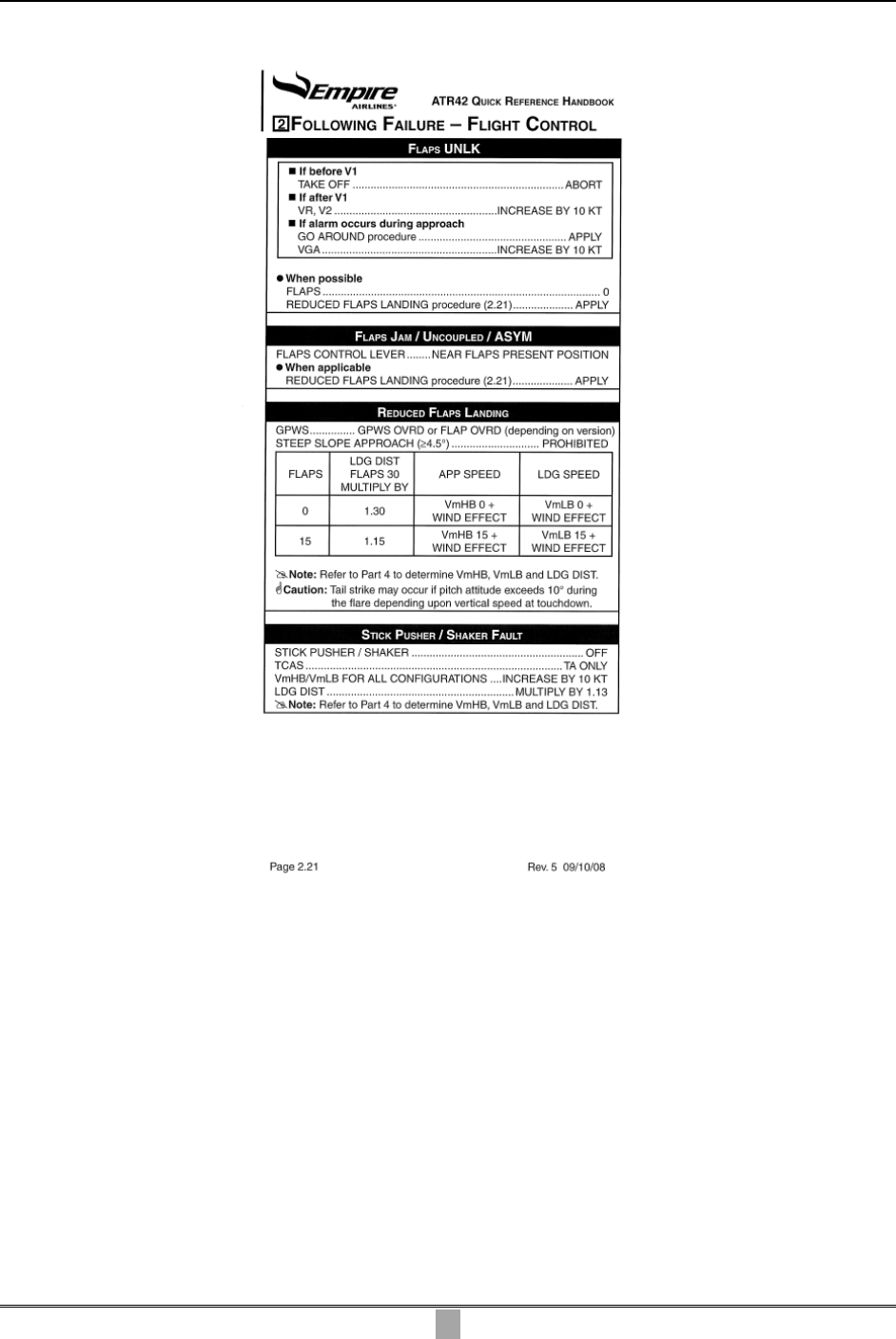
NTSB Aircraft Accident Report
Figure 7. Quick reference handbook page 2.21 with “FLAPS JAM/UNCOUPLED/ASYM” and
“REDUCED FLAPS LANDING” procedures.
According to the GOM, section 6-19, “Completion of Non-Normal Cockpit Checklist,”
flight crews are instructed that, “in the event of inoperative or malfunctioning flight control
system, if the airplane is controllable, complete only the applicable checklist procedures and do
not attempt any corrective action beyond those specified.” The GOM, section 6-4, “Circuit
Breakers Resetting,” stated that “tripped circuit breakers should not be reset in flight unless, in
the judgment of the PIC, it is necessary for the safe completion of the flight.”
The QRH, page 0.02 (directly beneath the Table of Contents), states the following
general information under the heading, “Procedures Initiation”:
28
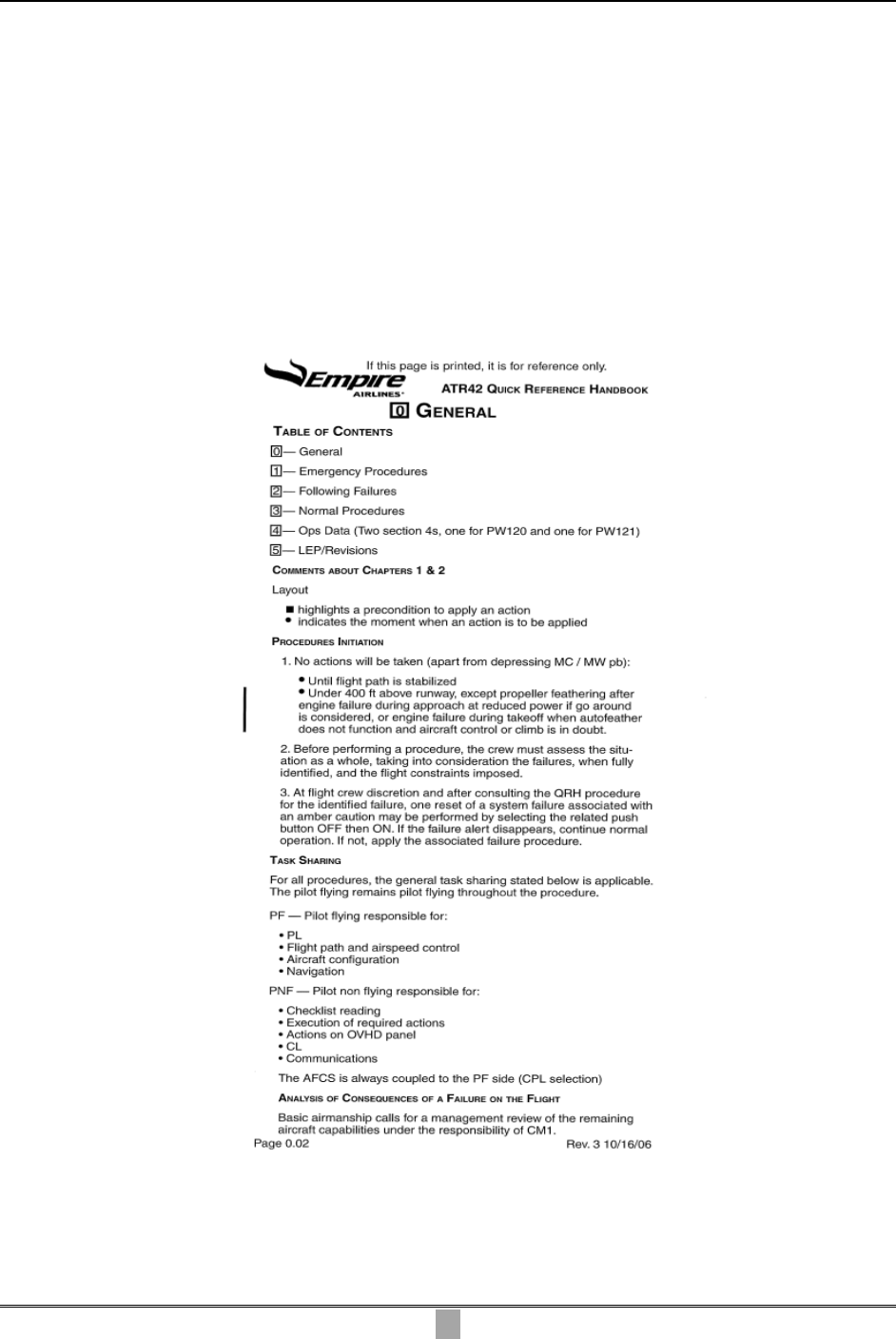
NTSB Aircraft Accident Report
… No actions will be taken…until the flight path is stabilized… . Before
performing a procedure, the crew must assess the situation as a whole, taking into
consideration the failures, when fully identified, and the flight constraints
imposed.
Page 0.02 of the QRH also states that the PF is responsible for the engine power levers,
flightpath and airspeed control, aircraft configuration, and navigation, and the PM is responsible
for completing the appropriate checklist items, the actions on the overhead panel, the positioning
of the condition levers (which relate to propeller control), and communications. Figure 8 shows
the general information on page 0.02 of the QRH.
Figure 8. General information on page 0.02 of quick reference handbook.
29

NTSB Aircraft Accident Report
30
Both the captain and the first officer received training on flap anomalies during ground
school and simulator training at FlightSafety. The flap system anomalies that were covered
during ground school training included flap jam, flap unlock, flap uncoupled, flap asymmetry,
and no flaps. Flap control circuit breakers were discussed. The ground training reviewed the
QRH for flap anomalies item by item. For a flap asymmetry, the training taught the pilots that
the airplane will try to roll, which requires the pilot to take the controls. During simulator
training, flap anomalies were covered as part of both initial and recurrent training. The type of
anomaly was given at the discretion of the instructor (the syllabus did not specify which anomaly
to present). Pilots were trained to look at the flap position indicator in the cockpit, and they were
also taught to look out the side windows at the flap position fairings to verify the flap
conditions.
47
The NTSB interviewed FlightSafety instructors who stated that, regardless of which
anomaly was presented and when, the response procedure was the same. The pilots were taught
to initiate a go-around maneuver and complete the QRH, which required them to rebug the
airspeeds for the flap setting that they had. During postaccident interviews, the FlightSafety
instructors, the FAA principal operations inspector (POI) for Empire Airlines, Empire Airlines’
chief pilot, and Empire Airlines’ director of operations indicated that they would have expected
the accident flight crew to use the QRH procedure in response to the flap anomaly. During
subsequent testimony at an NTSB public hearing,
48
Empire Airlines’ chief pilot and director of
operations both stated that they would have expected the flight crewmembers to first assess the
situation and then reference the QRH after identifing the problem.
FlightSafety did not train pilots to troubleshoot a flap anomaly by checking the circuit
breakers, and none of the instructors who were interviewed had ever observed a trainee attempt
to do so in the flight simulator. One instructor could not recall any pilots ever attempting to land
with a flap abnormality during training and stated that it was “drilled into their heads to go
around” if a flap problem occurred.
During postaccident interviews and public hearing testimony, the captain stated that he
checked the cockpit flap position indicator and determined that the flaps had not extended. He
also stated that he attempted to troubleshoot the flap problem by checking the circuit breakers
because he “had to start somewhere” and that he needed to determine what the malfunction was
and then handle it with the checklist. The captain stated that he did not follow the abnormal
procedures checklist for the flaps because the airplane was on a short final approach, things were
happening quickly, and he “was too busy and did not know which checklist to run first or the
speeds.”
During postaccident interviews and public hearing testimony, the first officer stated that
she did not know there was a flap asymmetry and thought they had no flaps. She further stated
that she was “a little bit” concerned about the captain’s use of a flashlight to look at the circuit
breakers during the approach. She also stated that she thought he should have been more focused
on landing the airplane. The first officer stated that, had they executed a missed approach, they
47
Verifying the flap conditions was simulated in training as there were no actual flap position fairings in the
simulator.
48
For more information about the public hearing, see Appendix A.
NTSB Aircraft Accident Report
31
would have had time to use the QRH, get situated, and set their airspeeds. The first officer stated
that, after the captain decided that the approach would be continued, there was not enough time
to use the QRH.
1.17.1.2 Stabilized Approach and Go Around
Empire Airlines’ ATR 42 pilot handbook and flight training manual (FTM) both
addressed stabilized approach criteria and approach standardization procedures. According to the
FTM, approaches conducted in IMC should be stabilized by 1,000 feet in height above
touchdown, and approaches conducted in visual meteorological conditions (VMC) should be
stabilized by 500 feet in height above touchdown.
The FTM listed several criteria for the flight crew to determine that an approach would
be considered stabilized. These criteria included (but were not limited to) ensuring that only
small changes in heading and pitch are needed to maintain the correct track, the rate of descent
deviates no more than plus or minus 300 fpm from the target descent rate, the airplane’s airspeed
is not less than the required approach speed, the maximum sink rate does not exceed 1,000 fpm
(a special briefing should be performed for any approach requiring a greater sink rate), the power
setting is appropriate for the configuration, and all briefings and checklists had been performed.
According to the ATR 42 pilot handbook, “Flight Profiles & Briefings,” the “Descent and
Approach Awareness Procedures” indicated that, during an ILS approach, the PM is to “call out
any deviations from normal altitude, airspeed, or descent rates throughout the approach.” The
procedures noted that the “captain calls for ‘missed approach,’ if necessary.” The pilot
handbook, section 2-02-04, stated that, if a go-around maneuver is required, the PF should
initiate the procedure by calling out “go around,” pressing the “GA” (go around) button on the
engine power levers, advancing the engine power levers toward the white mark, and calling out
“max power, flaps 15.”
FlightSafety instructors who were interviewed stated that stick-shaker activation meets
the criteria for an unstabilized approach. During postaccident interviews, the captain stated that
he was trained to go around if a problem occurs during approach and that his decision to
continue the approach was based on the runway conditions,
49
icing conditions, and the flap
problem. The captain stated that he “made a judgment call not to go around because things
started piling up, and it was better to land than to go around.” He stated that he “just wanted to
land as soon as possible.”
During a postaccident interview, the first officer stated that stick-shaker activation
“would be a go-around situation” and that she asked the captain about going around because the
company policy following stick shaker was to perform a go-around maneuver. The first officer
49
According to the CVR transcript, the LBB approach controller advised the flight crew that the Mu readings
(friction coefficient values taken by runway friction-measuring equipment) for runway 35L at touchdown, midpoint,
and rollout were .24, .25, and .23, respectively. The captain acknowledged and then advised the first officer that,
during landing, she should keep the airplane on the runway centerline and not touch the brakes. Empire Airlines’
GOM (section 6-12, revision 43) provided a table that “converts braking action reports to friction coefficient values”
and showed that Mu readings between .19 and .34 corresponded with a “poor” braking action report. The GOM also
stated that “there is no direct correlation between friction coefficient values and braking action” and that flight crews
should use the values “together with other knowledge, including recent braking action reports and wind conditions.”

NTSB Aircraft Accident Report
indicated that asking was her way of saying that she wanted to go around “without stepping on
toes.” The first officer further stated that she did not challenge the captain’s decision to continue
because she felt that he had a good reason for not wanting to go around and that she trusted that
he was making the right decisions. The first officer also stated that, after the captain took control
of the airplane, she thought that she should have suggested again that they go around and that she
did not know why she did not say anything.
1.17.1.3 Terrain Awareness and Warning System
According to the GOM, if the flight crew receives a TAWS caution alert or warning in
conditions other than daylight VMC (in which the flight crew can positively confirm that a
collision with the terrain will not take place), the flight crew is to “react immediately.” The
procedures for responding to a “pull up” warning stated that the flight crew is to advance to
go-around power, disconnect the autopilot, level the wings while simultaneously executing a
positive pull up, set flaps to the go-around position, retract the landing gear, and maintain the
specified minimum airspeed
until terrain clearance is assured.
1.17.1.4 Airspeed Bugs
As described in section 1.6.4.1, Empire Airlines’ ATR 42 pilot handbook stated that, for
an approach in icing conditions, the flight crew should set the internal, yellow, white, and red
bugs to correspond with the V
mHB
30 icing, V
ga
, V
mLB
0 normal, and V
mLB
0 icing airspeeds,
respectively. Flight crews were provided with an ATR 42 V-speed card pack that provided the
applicable minimum approach airspeeds based on the airplane’s weight. The same card that
provided approach airspeeds for each referenced airplane weight also provided airspeeds for use
during takeoff. The guidance provided to flight crews on setting the airspeed bugs did not
include any crosscheck procedures for verifying the information.
Postaccident examination of the cockpit found that the V-speed card pack was open to the
reference card for an airplane at 33,000 lbs gross weight. This card showed that, for this airplane
gross weight in icing conditions, V
mHB
30 was 116 kts, V
mLB
0 normal was 123 kts, and V
mLB
0
icing was 143 kts. V
ga
was not depicted on the card. According to the ATR 42 pilot handbook,
V
ga
is computed based on the normal approach airspeed (by either adding 5 kts to V
mHB
30 or
using 1.1 V
mca
, whichever is greater). Based on the card information, the approach airspeeds for
setting the internal, yellow, white, and red bugs were 116, 121, 123, and 143 kts, respectively,
and the takeoff airspeeds for setting the internal, yellow, white, and red bugs were 106, 112, 123,
and 143 kts, respectively.
According to the CVR transcript, during the captain’s approach briefing, he referenced
the “three thirty card” and read “one oh six [106 kts] is the icing speed…one oh six [106 kts] one
twelve [112 kts]…uh twenty three [123 kts] and forty three [143 kts].” Postaccident examination
of the captain’s and first officer’s airspeed indicators found that the captain’s internal, yellow,
white, and red bugs were set to 109, 110, 124, and 145 kts, respectively, and that the first
officer’s were set to 106, 112, 126, and 144 kts, respectively.
32
NTSB Aircraft Accident Report
33
1.17.1.5 Aileron Mistrim with Autopilot Engaged
With the autopilot system engaged, the roll anomaly induced by a flap asymmetry will
generate “RETRIM ROLL R [or L] WING DN” and “AILERON MISTRIM” messages on the
ADU. According to the manufacturer, a flight crew’s response to these messages should be to
hold the control wheel firmly, disengage the autopilot, and adjust the lateral trims. Upon
completion of these items, the autopilot may be reengaged. The AFM stated that, since the
autopilot may mask tactile cues that indicate adverse changes in airplane handling
characteristics, use of the autopilot is prohibited when unusual lateral trim requirements or
autopilot trim warnings are encountered when the airplane is in icing conditions.
50
During
postaccident interviews, both the captain and the first officer indicated that they did not see any
messages on the ADU.
1.17.1.6 Deicing and Anti-Icing Systems
The AFM defined three levels of icing equipment use and stated that level 3 protection,
which the flight crew used during the accident descent, should be used any time that ice is
observed accumulating on the airframe. According to the AFM, level 3 icing protection includes
all level 1 and 2 items, plus the use of continuous relight engine ignition and the airframe
pneumatic deicing boots.
51
Flight crew selection of the flight control horn anti-icing system
(used in level 2 and 3 ice protection) lowers the AOA stall warning threshold and triggers the
illumination of the green ICING AOA annunciator. Once airframe pneumatic boot use is selected
by the flight crew (by pushing the “AIRFRAME” button), the boot system inflates in sequence
continuously without further crew input.
According to the FCOM, the AAS’s amber ICING annunciator illuminates as soon as
(and as long as) the system’s ice detector senses that ice is building up. The flight crew was
trained to respond to AAS annunciators in the cockpit by increasing the minimum maneuvering
and operating airspeeds and selecting the anti-icing system when flying in icing conditions,
selecting the deicing system at the first indication of airframe ice accumulation, and switching
the deicing system off once ice is no longer present on the airframe. Once the ice detector no
longer senses that ice is accumulating, the system triggers the blue DEICING annunciator to
flash, alerting the flight crew to visually check for the absence of ice and determine if the deicing
system should be turned off.
The FCOM cautions that freezing rain is composed of SLD that may transform into clear
ice when it impacts the airplane’s skin in below-freezing temperatures. The FCOM states that
these large droplets may not freeze immediately upon impact and that the ice detector may
become “inefficient” (ineffective). According to ATR’s Cold Weather Operations publication,
52
50
The AFM also stated that use of the autopilot is prohibited any time that severe icing exists.
51
Level 1 protection, which was to be used during all flights, included use of the probe heat and windshield
heat. Level 2 protection, which was to be used for all takeoffs and all flight operations in atmospheric icing
conditions, included the level 1 items plus the use of propeller, flight control horn, and side window heat; engine
inertial separators and pneumatic boots; minimum propeller speed of 86 percent; illumination of the AOA light; and
icing speeds bugged and observed.
52
ATR Flight Operations Services, Cold Weather Operations: Be Prepared for Icing (2008). This publication
was updated in March 2011, and the current edition can be obtained from ATR’s website

NTSB Aircraft Accident Report
34
flight crews can visually assess ice accumulation by observing the propeller spinners,
windshield, airframe leading edges, wipers, and side windows.
According to the AFM limitations, section 4-5, if severe icing conditions are encountered
in flight, the flight crew’s procedures include escaping the severe icing conditions and notifying
ATC
.
According to the AFM,
severe icing may result from environmental conditions outside of those for which
the airplane is certificated. Flight in freezing rain, freezing drizzle, or mixed icing
conditions (supercooled liquid water and ice crystals) may result in ice buildup on
protected surfaces exceeding the capabilities of the ice protection system or may
result in ice forming aft of the protected surfaces.
The AFM states that the visual cues to identify severe icing include “ice covering all or a
substantial part of the unheated portion of either side window,” and/or an “unexpected decrease
in speed or rate of climb,” and/or the following secondary indications:
• Water splashing and streaming on the windshield.
• Unusually extensive ice accreted on the airframe in areas not normally observed
to collect ice.
• Accumulation of ice on the lower surface of the wing aft of the protected area.
• Accumulation of ice on the propeller spinner farther aft than normally observed.
In a postaccident interview, the captain stated that the airplane had encountered
“moderate bordering on severe” rime ice at FL 180. He stated that he selected level 3 ice
protection and that he noticed that, during the icing encounter, the airplane was cruising at
180 KIAS, whereas it would typically cruise at 200 to 210 KIAS. He stated that he requested a
descent to 14,000 feet msl and that, during the descent, “substantial amounts of ice” came off the
airplane. He noted that some ice from that encounter was still on the airframe when the flight
started its descent to LBB. Further, in a postaccident interview, the first officer stated that the
airplane began to accumulate ice again as it descended through 6,000 feet msl. She recalled that
level 3 ice protection had been activated and that she could see ice adhering on the propeller
spinner.
1.17.1.7 Crew Resource Management
CRM is the effective use of all available resources, people, information, and equipment to
achieve safe and efficient flight operations.
53
CRM involves crewmembers incorporating and
synchronizing the tasks required of them in a correct and timely manner
54
and communicating
<http://www.atraircraft.com/content/media/downloads/coldweatheroperations_2011_20.pdf> (accessed April 14,
2011).
53
J. Lauber, “Resource Management in the Cockpit,” Air Line Pilot, vol. 53 (1984), pp. 20-23.
54
J.A. Cannon-Bowers Volpe and others, “Defining Team Competencies and Establishing Team Training
Requirements,” in R. Guzzo, E. Salas, & Associates, eds., Team Effectiveness and Decision Making in
Organizations (San Francisco: Jossey-Bass, 1995), pp. 333-380.
NTSB Aircraft Accident Report
35
and coordinating effectively. FlightSafety provided CRM training to Empire Airlines’
crewmembers during initial training, and CRM was reviewed during recurrent training.
The CRM training provided during the pilots’ initial training consisted of 2 days
(16 hours) in the classroom and included lectures, case study reviews, and breakout and team
building sessions with crewmembers. Lecture topics included command and leadership,
situational awareness, communication, decision making, error management, teamwork and
synergy, fatigue, risk assessment, and automation management. The CRM training materials
included two presentation slides on assertion that encouraged pilots to speak up with
“appropriate persistence until there is a clear resolution.” The FlightSafety ATR program
manager stated that Empire Airlines’ CRM training program did not include role-playing
exercises in the classroom training. During a postaccident interview, the first officer stated that
she could not recall what was presented during the 2-day CRM training course, including
whether or not assertiveness was addressed.
According to Empire Airlines’ FTM, the CRM review provided during recurrent training
was included within the “Crew Duties and Responsibilities” module and in “Flight Module 1.”
According to Empire Airlines’ FTM, section 8-1-6, applied CRM is monitored and practiced in
each flight simulator module. One FlightSafety instructor stated that CRM was evaluated
throughout the simulator training because the ATR 42 is a two-pilot airplane, and he stated that
he would point out CRM issues in real time if he felt that it was necessary. Another instructor
indicated that instructors had the tools and techniques to teach CRM during the prebriefing, in
the simulator, and during the debriefing.
1.17.1.8 Weather Information and Training
Empire Airlines’ chief pilot indicated that, during basic indoctrination training, pilots
reviewed Empire Airlines’ aircraft deicing program (ADP); the FAA’s meteorology handbook;
the National Aeronautics and Space Administration’s (NASA) video, Tailplane Icing;
55
an
operations in icing for corporate aircraft video; and handouts of flight releases to familiarize
pilots with the format.
Empire Airlines’ chief pilot also indicated his belief that, during training at FlightSafety,
pilots reviewed the ATR Cold Weather Operations publication
56
and discussed meteorological
conditions likely to cause freezing drizzle and freezing rain. Interviews with FlightSafety
instructors revealed that several were familiar with the ATR publication but that none of the
instructors provided or discussed it during training. A review of Empire Airlines’ FTM revealed
that it included a task-listing document that indicated that Empire Airlines (not FlightSafety) was
55
The NASA video describes the tailplane stall condition that can result from horizontal stabilizer icing, its
warning signs, and the suggested recovery procedures. The video’s recovery procedures apply to airplanes that have
unpowered controls, that is, airplanes with horizontal stabilizers that have a fixed leading edge and movable elevator
surfaces that rely on aerodynamic balance to keep the control forces neutral. The ATR 42 is equipped with such
unpowered controls (also known as reversible controls). All airplanes that are certificated under 14 CFR Part 25
have been tested for tailplane stall susceptibility under at least the Part 25, Appendix C, icing conditions and have
demonstrated that they can be safely operated in such conditions. For conditions that are outside the Part 25,
Appendix C, icing envelope, the performance and handling characteristics of the airplanes are not required to have
been evaluated.
56
Cold Weather Operations: Be Prepared for Icing (2008).

NTSB Aircraft Accident Report
36
to provide the required training as part of the meteorology module, but Empire Airlines did not
provide it.
A review of the ATR Cold Weather Operations publication
57
revealed that it provided
guidance that advised pilots that icing is a major concern for commuter aircraft. The publication
stated that, due to their typical operating altitudes and airspeeds, turboprop aircraft fly where
icing conditions are most likely to occur. The publication also provided information about icing
meteorological phenomena, aircraft systems available to prevent and control ice accumulation,
aircraft performance loss due to ice contamination on the aerodynamic surfaces of the airplane,
and the procedures to apply on the ground and during flight when faced with icing conditions.
1.17.1.9 Stall and Near-Stall Recoveries
A review of Empire Airlines’ FTM revealed that company pilots were taught that at first
stall indication,
58
they should set maximum power, reduce pitch, roll wings level, and then,
during stall recovery, return to the entry altitude.
In June 2010, a stall recovery procedure was added to the ATR 42 AFM. The procedure,
“RECOVERY AFTER STALL OR UNCOMMANDED ROLL CONTROL,” specifies that the
pilot should push firmly on the control wheel and then set maximum power.
1.17.2 Aircraft Deicing Program (Ground)
In accordance with 14 CFR 121.629, Empire Airlines had an FAA-approved ADP to
address procedures for ensuring that no airplanes are dispatched or released for takeoff with
unsafe frozen contaminants on their surfaces. The program conformed to the guidance in
AC 120-60B, “Ground Deicing and Anti-Icing Program,” which provides information on
industry standards and practices related to ground deicing and anti-icing programs. The ADP
contained holdover tables that provided guidelines on the amount of time that deicing and
anti-icing fluid would protect an airplane’s critical surfaces from frozen contaminants, such as
active frost, freezing fog, snow, snow grains, freezing drizzle, light freezing rain, and rain on
cold-soaked wings.
1.17.3 Flight Dispatch
Empire Airlines’ flight dispatching functions were performed from the communications
center at its headquarters. As a 14 CFR Part 121 supplemental air carrier, Empire Airlines was
authorized to use flight followers (rather than licensed dispatchers) to authorize each flight
release, provide the necessary preflight weather products, and perform flight following of the
flight to the destination. All of Empire Airlines’ flight followers (with the exception of one who
57
Cold Weather Operations: Be Prepared for Icing (2008).
58
As defined by Empire Airlines, the first indication of a stall is the recognition by the pilot of the stall warning
aural “cricket,” the stick shaker, the stick pusher, or buffeting/lateral instability.

NTSB Aircraft Accident Report
37
was newly hired) were licensed dispatchers.
59
Flight followers communicated with flight crews
through the use of telephones, fax machines, and air-to-ground communications services.
The flight release for the accident flight was issued about 0211 and listed Roswell
International Air Center Airport, Roswell, New Mexico (located about 137 miles west of LBB),
as the alternate airport. The weather document indicated that the aviation routine weather reports
for LBB were reporting IFR conditions with light freezing drizzle and mist and that the aviation
terminal forecast expected the IFR conditions and light freezing drizzle to continue beyond the
estimated time of arrival. Several observations surrounding LBB also reported mixed freezing
precipitation across the area and indicated that these were not isolated events. The document also
contained the full AIRMET Zulu series (which pertains to icing) current over the area for
occasional moderate icing conditions below 22,000 feet msl. The document indicated that the
forecast for the Roswell International Air Center Airport expected wind from the north-northwest
at 12 kts, visibility better than 6 miles, no precipitation, and a ceiling broken at 1,600 feet agl.
According to the GOM, section 8-9, “when light freezing rain, light or moderate freezing
drizzle, or light, moderate or heavy snow is falling, aircraft may land.” The GOM also stated
that, “when light freezing rain, light to moderate freezing drizzle, or light, moderate snow is
falling, [an ATR] aircraft may take off, provided it is prepared in accordance with approved
deicing procedures.”
60
Empire Airlines’ director of operations stated that the airline developed
this guidance using the titles from the ADP holdover tables after receiving flight crew requests
for guidance related to operating in icing conditions.
During a postaccident interview, the flight follower who initiated preparations of the
flight release for the MAF-to-LBB flight leg indicated that she was aware of the freezing drizzle
conditions surrounding LBB. Another flight follower released the flight. The flight followers
who handled the accident flight’s release and the dispatch manager indicated that the GOM
contained no restriction that prevented ATR airplanes from operating in light freezing drizzle
and light freezing rain. All of them indicated that they believed that the ATR airplanes could
handle light freezing rain and freezing drizzle conditions but that the Cessna 208 airplanes
(which the flight followers indicated were prohibited from operating in those conditions) could
not. Both the dispatch manager and one of the flight followers indicated that as long as the
airplanes met the requirements for ground deicing, they could be released for flight.
During postaccident interviews, both the captain and the first officer stated that the
company did not pressure them to depart or arrive on time. The flight follower who released the
accident flight indicated that he had a “normal conversation” with the captain and that the
weather conditions were not that bad compared to other weather he had seen over the years. The
flight followers who were interviewed indicated that, if a captain disagreed with the flight
followers, the flight followers typically backed up the captain’s decision, and the captain had the
final say. During public hearing testimony, Empire Airlines’ manager of dispatch stated that if a
59
Although the flight followers were licensed dispatchers, their duties were defined more closely with the role
of flight follower and did not require the same initial and recurrent training that is required of a dispatcher.
60
The GOM prohibited the company’s Cessna 208 airplanes from departing, operating en route, or landing in
freezing rain or freezing drizzle of any intensity.

NTSB Aircraft Accident Report
38
captain was not comfortable launching due to weather, the flight follower would support the
captain’s decision.
A cursory review of other 14 CFR Part 121 and 135 operators’ icing guidance (which
included some operators that operated ATR or other turbine-powered, deice boot-equipped
airplanes) revealed that the guidance ranged from prohibitive to permissive. For example, some
guidance stated that “flight” or “takeoffs” in freezing rain and freezing drizzle was “not
approved” or “prohibited”; other guidance warned that “flight in freezing rain [or] freezing
drizzle…may result in ice buildup…exceeding the capability of the ice protection system” or that
“visible rain at temperatures below 0° C” may be conducive to “severe in-flight icing”; and other
guidance indicated that “aircraft may operate when light freezing rain [or] light to moderate
freezing drizzle…is falling…provided that it is prepared in accordance with approved deicing
procedures” or that “when light freezing rain [or] light or moderate freezing drizzle…is falling,
aircraft may land.”
1.17.4 Hazardous Materials
The GOM contains Empire Airlines’ procedures related to HAZMAT cargo. Specifically,
section 10-16 states that emergency response information (required in accordance with 49 CFR
172.600[c]) for use in mitigating an incident involving the HAZMAT cargo must be immediately
available where the HAZMAT is received, stored, or handled during transportation and must be
immediately available on board the aircraft. Section 10-17 indicates that, before departure, the
PIC must be provided written information about the HAZMAT cargo, proper shipping name,
hazard class, identification number, quantity, and location on board the airplane. The GOM
states that a copy of the HAZMAT document provided to the PIC is subject to the following (in
accordance with 49 CFR 175.33[c]):
This information must be readily accessible at the airport of departure and the
intended airport of arrival for the duration of the flight leg and [must be made…]
immediately available to any representative of federal, state, or local government
agency who is responding to an incident involving the flight.
1.17.5 Federal Aviation Administration Oversight
The FAA’s flight standards district office (FSDO) in Spokane, Washington, provided
oversight for Empire Airlines. The FSDO’s oversight of Empire Airlines’ 14 CFR Part 121
operations was managed through the FAA’s air transportation oversight system (ATOS).
According to the FAA, ATOS provides a means of oversight that allows air carriers to meet and
address all regulatory requirements, enables FAA inspectors to develop methodology for
continued operational safety, and provides FAA inspectors and air carriers the ability to manage
risk. The ATOS oversight requirements included oversight of the content of an airline’s manual
and the training of the flight crewmembers.
61
61
ATOS oversight requirements are contained in FAA Order 8900.1, Flight Standards Information
Management System, Volume 10, Chapter 1, Figure 10-7,“System/Subsystem/Element Chart—Operations and
Cabin Safety Elements.” Information obtained from the FAA’s website
<http://fsims.faa.gov/PICResults.aspx?mode=EBookContents> (accessed April 14, 2011).
NTSB Aircraft Accident Report
39
The FAA POI for Empire Airlines had been assigned to the company for more than
11 years. He stated that the GOM was the FAA-approved manual and that the pilot handbook
was “accepted.” He stated that he was the POI for the company when operations in freezing
drizzle were approved. He also stated that Empire Airlines had recently developed an internal
audit program for flight operations. The POI described Empire Airlines as a company with good
management people who self-report any problems.
The FAA principal maintenance inspector (PMI) for Empire Airlines had been assigned
to the company since 2000. He described Empire Airlines as very cooperative, very responsive in
correcting any identified problems, and consistent about submitting self-disclosures. The PMI
stated that his work program had been managed through ATOS since October 2006. He stated
that the ATOS process enabled him to develop the depth of inspection required.
1.17.6 Previous Accidents
The company had two previous fatal accidents in 1995 and 2000, both of which involved
single-pilot cargo flights that were operated under 14 CFR Part 135. On January 11, 1995, a
FedEx-owned Cessna 208 operated by Empire Airlines collided with a ridgeline in Pleasanton,
California, while it was cleared for a visual approach to the Metropolitan Oakland International
Airport, Oakland, California.
62
The NTSB determined that the probable cause of the accident
was the pilot’s failure to maintain both visual contact with terrain and sufficient altitude for
terrain clearance.
63
On October 9, 2000, a FedEx-owned Cessna 208 operated by Empire
Airlines collided with wooded terrain in Lummi Island, Washington, during a flight conducted in
IMC under a special visual flight rules (SVFR) clearance.
64
The NTSB determined that the
probable cause of the accident was the pilot’s attempted flight into known adverse weather
conditions and the pilot’s subsequent failure to maintain altitude above or clearance from the
trees.
65
62
The report for this accident, NTSB case number LAX95FA076, is available online at
<http://www.ntsb.gov/aviationquery/index.aspx>.
63
Contributing to the accident were the pilot’s decision to initiate a descent 14 miles from the airport and the
weather, specifically the cloud conditions and darkness.
64
The FAA defines SVFR conditions as meteorological conditions that are less than those required for basic
visual flight rules flight in controlled airspace. SVFR operations must be requested by the pilot and approved by
ATC. According to the accident report, the accident flight’s leg could not be conducted under IFR because there was
no published instrument approach procedure at the destination airport in Eastsound, Washington. The report for this
accident, NTSB case number SEA01FA001, is available online at <http://www.ntsb.gov/aviationquery/index.aspx>.
65
Contributing to the accident were the low ceilings, fog, the pilot’s low-altitude flight, rising terrain, and trees.

NTSB Aircraft Accident Report
40
1.18 Additional Information
1.18.1 Postaccident Safety Action
1.18.1.1 Federal Aviation Administration
Safety Alert for Operators: In-Flight Icing Operations and Training
On March 16, 2010, the FAA issued Safety Alert for Operators (SAFO) 10006, “In-Flight
Icing Operations and Training Recommendations,” to encourage all operators to review and
amend, if necessary, their flight crewmember and dispatcher training programs to ensure that
their programs address SLD icing conditions. The SAFO notes that SLD conditions, which the
FAA considers synonymous with freezing drizzle and freezing rain aloft, are “icing conditions
containing droplets larger than those required to be demonstrated in aircraft icing certification
criteria. SLD may result in ice formation beyond the capabilities of the airplane’s ice protection
system to provide adequate ice protection.”
The SAFO referenced the NTSB’s investigation of the October 31, 1994, accident
involving an ATR 72-212 that crashed following an in-flight encounter with icing in Roselawn,
Indiana.
66
In the SAFO, the FAA recommended that the directors of safety and directors of
operations for 14 CFR Part 121 and 135 operators and the training managers for all operators
ensure that their training programs include a review of the following: meteorological conditions
likely to cause SLD conditions; identification of weather information sources (such as AIRMET,
significant meteorological information [SIGMET], center weather advisories, hazardous in-flight
weather advisory service, current icing potential, and forecast icing potential) and their use as it
relates to flight crewmembers’ and dispatchers’ preflight planning and in-flight decision making;
discussion of company and ATC procedures for pilot reports on severe icing; discussion of flight
crewmembers’ identification of severe icing conditions associated with freezing rain and
freezing drizzle, including immediate exit procedures and ATC procedures should severe icing
be encountered; and a review of the FAA publication, “Roll Upset in Severe Icing.”
67
Proposed Rulemaking for Airplane Certification Requirements for Flight in Icing
Conditions
On June 29, 2010, in response to several NTSB safety recommendations (several of
which were issued during the NTSB’s investigation of the October 31, 1994, accident in
Roselawn, Indiana,
68
and many of which superseded or expanded upon previous safety
recommendations issued in 1981),
69
the FAA issued a notice of proposed rulemaking (NPRM),
66
See In-flight Icing Encounter and Loss of Control, Simmons Airlines, d.b.a. American Eagle Flight 4184,
Avions de Transport Regional (ATR) Model 72-212, N401AM, Roselawn, Indiana, October 31, 1994; Volume 1:
Safety Board Report (Revision 9/13/02), Aircraft Accident Report NTSB/AAR-96/01 (Washington, DC: National
Transportation Safety Board, 1996). <http://www.ntsb.gov/publictn/1996/AAR9601.pdf>.
67
“Roll Upset in Severe Icing,” Flight Safety Digest (January 1996). Information obtained from the Flight
Safety Foundation’s website <http://flightsafety.org/fsd/fsd_jan96.pdf> (accessed March 21, 2011).
68
NTSB/AAR-96/01.
69
The NTSB first identified the need for the FAA to review and revise the icing criteria in 14 CFR Part 25,
Appendix C, in a 1981 safety report. For more information, see Aircraft Icing Avoidance and Protection,
September 9, 1981, Safety Report NTSB/SR-81/01 (Washington, DC: National Transportation Safety Board, 1981).
NTSB Aircraft Accident Report
41
“Airplane and Engine Certification Requirements in Supercooled Large Drop, Mixed Phase, and
Ice Crystal Icing Conditions,” intended to improve the safety of transport-category airplanes
operating in SLD, mixed-phase, and ice-crystal icing conditions.
70
Included in the NPRM were
proposals for expanding the certification icing environment for transport-category airplanes to
include freezing rain and freezing drizzle and to require airplanes most affected by SLD icing
conditions to meet certain safety standards in the expanded certification icing environment,
including additional airplane performance and handling requirements. The NPRM noted that
freezing drizzle is outside the icing envelope
71
currently specified in 14 CFR Part 25,
Appendix C, which contains the certification requirements for transport-category airplanes.
72
1.18.1.2 Empire Airlines
On March 17, 2009, Empire Airlines’ Director of Flight Operations wrote an email to
NTSB investigators detailing the company’s postaccident actions. These actions included the
following:
Training Guidance for Flap Anomalies
Empire Airlines distributed guidance to all check airmen and the FlightSafety ATR
program manager that stated the following:
In the course of conducting flight training or checking in the ATR (airplane or
simulator) and specifically while executing flap malfunction and reduced flap
landing, do not let the crew think that you want them to continue the approach
without taking the time to complete the QRH procedure(s), reset the speed bugs,
rebrief the approach, etc…Depending on where the crew recognizes the flap
problem, they should probably ask ATC (instructor/check airman) for a delay
vector or hold while they complete the QRH before continuing the approach. The
point is we don’t want to train or check differently than we want the crew to fly
the aircraft. We should expect them to delay the approach until all the QRH
procedures and briefs are complete.
Flight Information Bulletin for Airspeed Bugs
On February 23, 2009, Empire Airlines issued Flight Information Bulletin 09-01 to all
ATR crewmembers explaining the proper determination and setting of airspeed bugs for flight in
icing conditions. The company also added expanded procedures to the ATR pilot handbook for
flight crews to be aware of errors in setting airspeed bugs and added a procedure for the setting
and readback of the bugs during the departure and approach briefings.
70
75 Federal Register (FR) 37311-37339 (June 29, 2010).
71
According to the NPRM, the term “icing envelope” refers to “the environmental icing conditions within
which the airplane must be shown to be able to safely operate.”
72
For information about the NTSB’s August 27, 2010, comments to the FAA regarding the NPRM, see
section 2.4.1.2.

NTSB Aircraft Accident Report
42
Flight Operations Bulletin for Icing
On February 27, 2009, Empire Airlines issued Flight Operations Bulletin 09-04, which
contained information to supersede the information contained in the GOM, section 8-9, “Icing.”
The flight operations bulletin, which was intended for both ATR flight crews and flight
followers, included the following information:
Freezing rain…and freezing drizzle…are not covered by the certification icing
envelope as defined in Part 25, Appendix C. Takeoff or landing operations in
known or reported [freezing rain or freezing drizzle] of any intensity, are
prohibited.
Special Emphasis Icing Training
Empire Airlines implemented special emphasis icing training, which increased the time
spent during ground training for all ATR pilots and dispatchers and included a review of the
ATR Cold Weather Operations publication,
73
the NASA Tailplane Icing video, and the 14 CFR
Part 25, Appendix C, icing certification envelope. The training also included a review of SLD;
severe icing; icing reports, forecasts, advisories, AIRMETs, and SIGMETs; and a review of
aircraft performance and the recommended maximum crosswind and tailwind components with
respect to operations with contaminated runways.
1.18.1.3 FedEx Feeder Operations
In April 2009, FedEx facilitated a safety summit with its feeder operators to address the
circumstances of this accident and facilitate training improvement and adherence to best
practices. As a result of the safety summit, the ATR training curriculum taught at FlightSafety
was modified to include stick-shaker and stick-pusher recognition and recovery training, special
purpose operational training, and line-oriented flight training (one module of which is still under
development). ATR initial training was also increased with two sessions added. In addition,
company instructors were placed on site at FlightSafety to perform company-specific training
and check rides to complement FlightSafety’s instruction.
All FedEx feeder operators developed “no-go” weather items (similar to those contained
in Empire Airlines’ Flight Operations Bulletin 09-04) that prohibit takeoff or landing operations
in known or reported freezing rain or freezing drizzle. All of the operators have implemented
procedures for ensuring that airspeed bugs are properly used and verified during all phases of
flight. Ice evidence probes (IEPs) have been installed on all ATR airplanes that were not so
equipped (the installations were completed by October 2009).
73
Cold Weather Operations: Be Prepared for Icing (2008).
NTSB Aircraft Accident Report
43
1.18.2 Previously Issued Safety Recommendations
1.18.2.1 Flight Crew Monitoring and Workload Management Skills for Single and
Multiple Abnormal Situations
On February 23, 2010, as a result of its investigation of the February 12, 2009, accident
involving a Colgan Air (operating as Continental Connection) Bombardier DHC-8-400, which
crashed during an instrument approach in Buffalo, New York,
74
the NTSB issued Safety
Recommendation A-10-10, which asked the FAA to do the following:
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
review their standard operating procedures to verify that they are consistent with
the flight crew monitoring techniques described in Advisory Circular (AC)
120-71A, “Standard Operating Procedures for Flight Deck Crewmembers”; if the
procedures are found not to be consistent, revise the procedures according to the
AC guidance to promote effective monitoring.
On June 22, 2010, the FAA responded that it was considering options such as issuance of
a SAFO or an information for operators (InFO) bulletin to address this recommendation. On
January 25, 2011, the NTSB indicated that although such action may represent part of an
acceptable response to this recommendation, the FAA must also ensure that the guidance
provided in documents like SAFOs is implemented.
75
Pending the recommended actions, the
NTSB classified Safety Recommendation A-10-10 “Open—Acceptable Response.”
As a result of its investigation of the February 16, 2005, accident involving a Cessna
Citation 560 that crashed during an ILS approach in icing conditions,
76
the NTSB issued Safety
Recommendation A-07-13, which asked the FAA to do the following:
Require that all pilot training programs be modified to contain modules that teach
and emphasize monitoring skills and workload management and include
opportunities to practice and demonstrate proficiency in these areas.
74
In this accident, “the flight crew’s failure to monitor airspeed” was a contributing factor. See Loss of Control
on Approach, Colgan Air, Inc., Operating as Continental Connection Flight 3407, Bombardier DHC-8-400,
N200WQ, Clarence Center, New York, February 12, 2009, Aircraft Accident Report NTSB/AAR-10/01
(Washington, DC: National Transportation Safety Board, 2010).
<http://www.ntsb.gov/publictn/2010/AAR1001.pdf>.
75
At the same time Safety Recommendation A-10-10 was issued, the NTSB also issued Safety
Recommendation A-10-31, which concerns the need to ensure that guidance provided in documents like SAFOs has
been implemented. Safety Recommendation A-10-31 asked the FAA to do the following: “Implement a process to
document that all 14 Code of Federal Regulations Part 121, 135, and 91K operators have taken appropriate action in
response to safety-critical information transmitted through the safety alert for operators process or another method.”
On January 25, 2011, the NTSB classified this recommendation “Open—Acceptable Response,” pending FAA
action.
76
The NTSB determined that the probable cause of the accident included “the flight crew’s failure to
effectively monitor and maintain airspeed.” See Crash During Approach to Landing, Circuit City Stores, Inc.,
Cessna Citation 560, N500AT, Pueblo, Colorado, February 16, 2005, Aircraft Accident Report NTSB/AAR-07/02
(Washington, DC: National Transportation Safety Board, 2007).
<http://www.ntsb.gov/ntsb/publictn/2007/AAR0702.pdf>.

NTSB Aircraft Accident Report
44
On May 17, 2007, the FAA stated that monitoring skills and workload management are
part of CRM and that current CRM regulations adequately address the issues in this
recommendation. However, the FAA indicated that it would consider identifying in its work
program a list of required inspections, reemphasizing to the regional and FSDO managers the
need to validate the training that is already required and verify its effectiveness. On September 9,
2008, the NTSB responded that the FAA’s list should include a strong emphasis on monitoring
and workload management components of the CRM program. On February 23, 2010, as a result
of the FAA’s lack of progress in response to the safety recommendation and the NTSB’s
subsequent investigation of the Colgan Air accident,
77
the NTSB reiterated A-07-13 and
classified it “Open—Unacceptable Response.”
On May 19, 2009, as a result of the NTSB’s investigation of the September 28, 2007,
accident involving American Airlines flight 1400, a McDonnell Douglas DC-9-82, which
experienced an in-flight engine fire and nose landing gear anomaly that presented the flight crew
with multiple, simultaneous emergency and abnormal situations,
78
the NTSB issued Safety
Recommendations A-09-24 and -25, which asked the FAA to do the following:
Establish best practices for conducting both single and multiple emergency and
abnormal situations training. (A-09-24)
Once the best practices for both single and multiple emergency and abnormal
situations training asked for in Safety Recommendation A-09-24 have been
established, require that these best practices be incorporated into all operators’
approved training programs. (A-09-25)
On August 11, 2009, the FAA responded that it supports “realistic, scenario-based
training that serves to develop pilot psychomotor skills as well as critical thinking and
decision-making abilities in response to the range of unusual or unanticipated events that may
occur during flight operations.” The FAA stated that, on January 12, 2009, it published an
NPRM, “Qualification, Service, and Use of Crewmembers and Aircraft Dispatchers,”
79
that
included such scenario-based training for all 14 CFR Part 121 operators. The FAA also indicated
that it planned to revise FAA Order 8900.1, “Flight Standards Information Management
System,” to require POIs to withdraw approval of any Part 121 training program that does not
include such training.
On April 2, 2010, the NTSB responded that, although issuance of the final rule proposed
in the NPRM would give the FAA the regulatory framework to require the training, the NTSB
remained concerned that, without a guide to best practices, inspectors and operators would have
difficulty creating effective programs. Pending the outcome of the FAA’s planned review of
regulatory and policy framework to determine whether additional guidance or requirements are
77
NTSB/AAR-10/01.
78
See In-Flight Left Engine Fire, American Airlines Flight 1400, McDonnell Douglas DC-9-82, N454AA,
St. Louis, Missouri, September 28, 2007, Aircraft Accident Report NTSB/AAR-09/03 (Washington, DC: National
Transportation Safety Board, 2009). <http://www.ntsb.gov/publictn/2009/AAR0903.pdf>.
79
74 FR 1280 (January 12, 2009).
NTSB Aircraft Accident Report
45
necessary, the NTSB classified Safety Recommendations A-09-24 and -25 “Open—Acceptable
Response.”
1.18.2.2 Go-Around Callout
During the NTSB’s investigation of the February 18, 2007, accident involving a Shuttle
America (doing business as Delta Connection) Embraer ERJ-170, which overran the runway
during landing,
80
the NTSB concluded that both the PF and the PM should have the authority to
call for a go-around maneuver because one pilot might detect a potentially unsafe condition of
which the other pilot is unaware. As a result, the NTSB issued Safety Recommendation A-08-18,
which asked the FAA to do the following:
Require 14 Code of Federal Regulations Part 121, 135, and Part 91 subpart K
operators to have a written policy emphasizing that either pilot can make a
go-around callout and that the response to the callout is an immediate missed
approach.
On September 26, 2008, the FAA responded that it would publish a SAFO that discusses
the hazards associated with cockpit crewmembers who do not immediately and instinctively
react to a go-around callout while on an approach for landing. The FAA also stated that it would
revise FAA Order 8900.1 to include guidance to POIs to have all 14 CFR Part 121, 135, and 91
subpart K operators develop written policy that indicates that either pilot can make a go-around
callout and that the response to the callout is an immediate missed approach.
On June 22, 2009, the NTSB indicated that, pending the FAA’s revision of
FAA Order 8900.1 and its completion of a survey to ensure that all operators have developed and
implemented the recommended policy, Safety Recommendation A-08-18 was classified
“Open—Acceptable Response.” On March 1, 2010, the FAA issued SAFO 10005, “Go-Around
Callout and Immediate Response,” which provided information to operators and recommended
that they provide written policy to flight crews regarding go-around callouts. The other requested
action items have not yet been completed.
1.18.2.3 Low-Airspeed Alerting Systems
As a result of the February 12, 2009, Colgan Air accident,
81
the NTSB issued Safety
Recommendation A-10-12, which superseded Safety Recommendations A-03-53 and -54
82
and
asked the FAA to do the following:
80
See Runway Overrun During Landing, Shuttle America, Inc., Doing Business as Delta Connection Flight
6448, Embraer ERJ-170, N862RW, Cleveland, Ohio, February 18, 2007, Aircraft Accident Report
NTSB/AAR-08/01 (Washington, DC: National Transportation Safety Board, 2008).
<http://www.ntsb.gov/publictn/2008/AAR0801.pdf>.
81
NTSB/AAR-10/01.
82
Safety Recommendations A-03-53 and -54, which were issued on December 2, 2003, were classified
“Closed—Unacceptable Action/Superseded” on February 23, 2010, because of a lack of progress. Safety
Recommendation A-03-53 asked the FAA to do the following: “Convene a panel of aircraft design, aviation
operations, and aviation human factors specialists, including representatives from the National Aeronautics and
NTSB Aircraft Accident Report
46
For all airplanes engaged in commercial operations under 14 Code of Federal
Regulations Parts 121, 135, and [Part 91 subpart] K, require the installation of
low-airspeed alert systems that provide pilots with redundant aural and visual
warnings of an impending hazardous low-speed condition.
On June 22, 2010, the FAA responded that it planned to task the Aviation Rulemaking
Advisory Committee (ARAC) with developing recommendations for potential requirements to
address low-airspeed alerting systems. On January 25, 2011, the NTSB acknowledged that
asking the ARAC to address the issue of low-airspeed alerting systems may represent the first
step in an acceptable response to this recommendation. However, due to the FAA’s lack of
progress in this area, the NTSB classified Safety Recommendation A-10-12 “Open—
Unacceptable Response,” pending substantive action by the ARAC to address this
recommendation.
1.18.2.4 First Officer Assertiveness
As a result of its investigation of the February 19, 1996, accident involving Continental
Airlines flight 1943, a Douglas DC-9-32, which landed wheels up,
83
the NTSB issued Safety
Recommendations A-97-05 and -06, which asked the FAA to do the following:
Require all principal operations inspectors of 14 CFR Part 121 carriers to ensure
that the carriers establish a policy and make it clear to their pilots that there will
be no negative repercussions for appropriate questioning in accordance with crew
resource management techniques of another pilot’s decision or action. (A-97-05)
Require all principal operations inspectors of 14 CFR Part 121 carriers to ensure
that crew resource management programs provide pilots with training in
recognizing the need for, and practice in presenting, clear and unambiguous
communications of flight-related concerns. (A-97-06)
On October 30, 1998, the FAA issued AC 120-51C (currently AC 120-51E), which
emphasized the importance of all levels of management to support a safety culture that promotes
communication by encouraging appropriate questioning and that there will be no negative
repercussions for appropriate questioning of one pilot’s decision or action by another. The NTSB
also requested that the FAA issue a flight standards information bulletin (FSIB) to provide
guidance to POIs to ensure that operators are complying with the information presented in
Space Administration, to determine whether a requirement for the installation of low-airspeed alert systems in
airplanes engaged in commercial operations under 14 Code of Federal Regulations Parts 121 and 135 would be
feasible, and submit a report of the panel’s findings.” Safety Recommendation A-03-54 asked the FAA to do the
following: “If the panel requested in Safety Recommendation A-03-53 determines that a requirement for the
installation of low-airspeed alert systems in airplanes engaged in commercial operations under 14 Code of Federal
Regulations Parts 121 and 135 is feasible, establish requirements for low-airspeed alert systems, based on the
findings of this panel.”
83
In this accident, the captain rejected, without any discussion, the first officer’s go-around request, and the
first officer failed to challenge his decision. See Wheels-Up Landing, Continental Airlines Flight 1943, Douglas
DC-9-32, N10556, Houston, Texas, February 19, 1996, Aircraft Accident Report NTSB/AAR-97/01 (Washington,
DC: National Transportation Safety Board, 1997). <http://www.ntsb.gov/publictn/1997/AAR9701.pdf>.

NTSB Aircraft Accident Report
47
AC 120-51C. Based on the lack of action by the FAA to issue the FSIB, on February 23, 2000,
the NTSB classified these recommendations “Closed—Unacceptable Action.”
1.18.3 Airplane Equipment Options
1.18.3.1 Aircraft Performance Monitoring System
Since November 2005, new production ATR 42 and ATR 72 airplanes have been
equipped with an aircraft performance monitoring (APM) system
84
designed to assist flight
crews with monitoring airplane performance during operations in icing conditions. According to
ATR’s Cold Weather Operations publication,
85
ATR developed the APM to enhance a flight
crew’s ability to detect severe icing conditions after finding that flight crews do not always
adequately monitor the cues and follow the procedures established for responding to severe icing
encounters. The APM uses FDR-recorded parameters and other information
86
to calculate and
compare the airplane’s actual performance (with respect to airspeed and drag) with its expected
performance. The APM also computes the actual minimum icing and severe icing airspeeds. The
APM function is included in the airplane’s multipurpose computer and requires no additional
sensors or any calculation of atmospheric ice content.
If the APM detects that the minimum airspeed requirements are not being met or that
degraded airplane performance is present, the APM alerts the flight crew via aural chimes and
annunciator lights on each pilot’s panel. The system is designed to provide these alerts only
when the static air temperature is below 10° C, the airplane’s flaps and landing gear are retracted,
both engines are operating, and level 2 or 3 icing protection is engaged or an icing signal is
provided by the ice detector.
During cruise flight, if the APM detects that the airplane’s indicated airspeed is 10 kts
lower than the expected value, the blue “CRUISE SPEED LOW” annunciator lights will
illuminate to alert the flight crew to monitor the icing conditions and airspeed.
87
During climb,
cruise, or descent, if the APM detects that the airplane’s performance is becoming degraded, the
amber “DEGRADED PERF” annunciator lights will illuminate with a single aural chime to alert
the flight crew to apply the appropriate QRH procedures to verify that the deicing protection is
on, maintain red-bug airspeed plus 10 kts, and check for severe icing cues or abnormal handling.
The QRH states that, if such cues are absent, the flight may be continued and that icing
conditions and airspeed should be monitored. If the APM detects that the airspeed decays further
and the minimum icing airspeed is reached, the amber “INCREASE SPEED” annunciator lights
will flash with a single aural chime to alert the flight crew to increase the airspeed.
According to ATR, had the accident airplane been equipped with an APM, the flight crew
would have received the blue “CRUISE SPEED LOW” annunciator lights after about 10 minutes
84
The modification began with ATR 42-500 SN 641 and ATR 72-212A SN 726. The accident airplane, which
was older, was not equipped with an APM.
85
Cold Weather Operations: Be Prepared for Icing (2008).
86
The APM also uses aircraft weight information that must be input by the flight crew.
87
The light will extinguish once the appropriate airspeed is maintained.

NTSB Aircraft Accident Report
48
of cruise flight in the icing conditions at FL 180. During the descent through about 5,000 feet
msl, the flight crew would have received the blue “CRUISE SPEED LOW” annunciator lights
about 70 seconds before they selected the flap extension and the amber “DEGRADED PERF”
annunciator lights and single chime about 40 seconds before they selected the flap extension.
After the flight crew selected the flap extension, an APM would have provided no further
annunciator lights or chimes because the system requires a flaps-up configuration.
After the APM system was first introduced, on October 12, 2005, the Direction Générale
de l’Aviation Civile (DGAC) of France issued Recommendation Bulletin 2005/31(B) to “inform
the concerned authorities and operators of the new design improvement” and to “strongly
recommend” that ATR operators install the APM on their ATR fleets; the FAA did not issue a
similar advisory. In the bulletin, DGAC indicated that “no unsafe condition exists” for airplanes
that are not equipped with an APM provided that the flight crew applies the appropriate
procedures for detecting and responding to a severe icing encounter. However, DGAC noted that
an APM can help flight crewmembers recognize when they enter severe icing conditions and can
help them respond appropriately to such an encounter. On December 11, 2006, ATR issued All
Operators Message 42-72/2006/08 to notify all operators of the availability of the APM retrofits
and to recommend their installation. ATR also provided operators with information about the
APM in various publications and at several flight operations conferences worldwide.
On August 10, 2009, the European Aviation Safety Agency (EASA) issued
AD 2009-0170, effective August 24, 2009, that required all EASA-participating operators
(operators in the European Community, its Member States, and the European third countries) of
ATR 42 and 72 airplanes not originally equipped with the APM system to retrofit their airplanes
with the system within 72 months or by the second “C” check,
88
whichever occurs first. The
FAA took no similar action. As a result, APM system retrofits are optional for U.S. operators of
ATR 42 and ATR 72 airplanes not originally equipped with the system. According to ATR, of
the 780 ATR 42 and ATR 72 airplanes in service worldwide, 250 are equipped with APMs. Of
the 90 ATR 42 and ATR 72 airplanes in the United States, none are equipped with APMs.
1.18.3.2 Flap Malfunction or Asymmetry Light
Several ATR airplanes, including all ATR 42-200, -300, and -320 models (like the
accident airplane), were certificated without a cockpit light for a flap asymmetry or malfunction.
The certification basis that applies to these airplanes includes 14 CFR 25.699,
89
which states the
following:
there must be a means to indicate to the pilots the position of each lift or drag
device having a separate control in the cockpit to adjust its position. In addition,
an indication of unsymmetrical operation or other malfunction…must be provided
88
A “C” check is a heavy maintenance inspection performed at intervals based on manufacturer-specified
airplane usage parameters.
89
According to EASA, the original certification basis for the ATR 42-320 was Joint Aviation Requirements,
change 8 for paragraph 25.699, which is similar in content to 14 CFR 25.699, amendment level 25-23, effective
May 8, 1970.

NTSB Aircraft Accident Report
49
when such indication is necessary to enable pilots to prevent or counteract an
unsafe flight…condition.
Certification testing demonstrated that a flap asymmetry in these airplanes (which is
limited to less than 10° by the airplanes’ flap asymmetry detection system)
90
did not constitute
an unsafe flight condition because the airplanes remained controllable. Later-model ATR
airplanes, including all ATR 42-400 and -500 and all ATR 72-101, -102, -201, -211, -212, and
-212A models, have a cockpit light that indicates a flap asymmetry. The airplane manufacturer
stated that the asymmetry light was added as part of an upgrade to the airplanes’ flight
management system. The flap asymmetry light was designed to illuminate amber any time that
an asymmetry greater than 6.7° occurred. Nearly all transport-category airplanes, with the
exception of the ATR 42-200, -300, and -320 models and the Cessna 500, 550, 553, 560, and
560XL models, are certificated with some type of flap malfunction indicator in the cockpit, some
of which specifically indicate flap asymmetry.
1.18.3.3 Ice Evidence Probe
Since 1995, new-production ATR airplanes have been equipped with an IEP, which is
mounted so that it is visible from the left-side cockpit window and is considered the primary
means for flight crews to monitor ice accumulation.
91
The IEP provides an airfoil-shaped surface
upon which ice accumulation can be visually detected and is designed to retain ice on its surface
until the entire aircraft is free of ice, thus helping flight crews determine when critical surfaces of
the airplane may be free of ice. The IEP is automatically illuminated for use during night
operations when the airplane’s navigation lights are turned on. For all ATR airplanes that were
not originally equipped with IEPs, ATR provided the operators with the service bulletin and kits
necessary for installing IEPs free of charge. These kits were distributed in 1995, and the
installation was optional.
The accident airplane was not equipped with an IEP.
90
FAA personnel indicated that most airplanes’ flap asymmetry detection systems are similar in that they limit
the amount of asymmetry that can occur.
91
Cold Weather Operations: Be Prepared for Icing (2008).

NTSB Aircraft Accident Report
50
2. Analysis
2.1 General
The captain and the first officer were certificated in accordance with Federal regulations
and were current and qualified in accordance with Empire Airlines’ training requirements. The
investigation found no evidence that the pilots’ performance was affected by any behavioral or
medical condition, or by the use of alcohol or drugs.
The airplane was loaded within weight and CG limits and was maintained in accordance
with 14 CFR Part 121. Although Empire Airlines could not immediately locate the left engine’s
AD records, work orders and other records were located that indicated the AD compliance items
had been performed. The investigation found no evidence that indicated any mechanical anomaly
with the engines, and FDR data indicated that the engines’ performance was consistent with
normal operations.
The flight experienced two separate periods of airframe ice accretion, the first during
cruise flight at FL 180 and the second during descent below 6,000 feet msl. The flight crew
selected ice protection during both icing encounters, and no evidence indicated any mechanical
anomalies with the airplane’s deicing and anti-icing systems. According to the captain, following
the first icing encounter, during the descent above 6,000 feet msl, “substantial amounts of ice”
came off the airplane. The shedding of ice is consistent with the presence of a layer of air with
temperatures above freezing between 6,000 and 11,000 feet msl due to a temperature inversion.
Further, performance calculations based on FDR data indicated that, during the descent between
14,000 to about 5,000 feet msl, the airplane’s performance was as expected for an ice-free
airframe. During the approach into LBB, the airplane began to accumulate ice again when it
descended into moderate icing conditions resulting from light freezing drizzle, a weather
condition that was outside its icing certification envelope as specified in 14 CFR Part 25,
Appendix C.
92
During the approach as the airplane descended through about 4,800 feet msl, the FDR
recorded that a flap asymmetry occurred about 1 second after the cockpit flap position lever was
positioned to command 15° flaps. The FDR recorded no operational anomalies with the
airplane’s hydraulic systems, and the flight crew reported none. Performance data indicated that,
when the flight crew commanded 15° flaps, a flap asymmetry occurred with the left flaps
extending 8° to 10° and the right flaps not extending. The data further indicated that the flaps
returned to a symmetric state (about 4.5°) about 25 seconds before ground impact.
Based on the circumstances of the accident flight, a number of scenarios could have
resulted in a flap asymmetry, and the investigation evaluated the possibility that a mechanical
anomaly, flap actuator jamming, mechanical restriction of the movement of the right flaps, or
hydraulic fluid contamination may have occurred. Postaccident impact and fire damage to the
right flaps limited the extent to which preimpact system integrity could be determined
92
For information about the NTSB’s longstanding concerns about the operation of airplanes in weather
conditions that are outside their icing certification envelope, see section 2.4.1.

NTSB Aircraft Accident Report
(components from the left flaps sustained less damage during the accident sequence and the left
flaps’ actuators functioned when tested). X-ray examinations and disassembly of all four flap
actuators (for both the left and right flaps) showed that their internal components were intact at
the time that the asymmetry occurred, that hydraulic fluid (or evidence of hydraulic fluid) was
present in each actuator, and that no evidence existed of any mechanical anomaly or jamming of
the actuators. Examination of the available components from the right flaps revealed no evidence
that any mechanical restriction of the movement of the flaps had occurred with respect to those
components (thermal damage precluded examination of the entire system).
According to ATR, ice formation on the flap surfaces could not result in a delayed
extension of the flaps because in all types of icing conditions, runback icing does not exceed 15
to 20 percent of the wing chord on the upper wing surface and 30 to 40 percent of the wing chord
on the lower wing surface and that these limits are upstream of the flaps. Further, ATR noted that
there were no reports of a flap asymmetry due to ice formation in the operational history of the
aircraft make/model. However, because the airplane was operating outside of its icing
certification envelope at the time of the accident and runback ice was found on the lower surface
of a separated section of the right aileron, the investigation could not rule out the possibility that
ice could have formed and either delayed or restricted the flap extension and resulted in a flap
asymmetry.
Testing of recovered hydraulic fluid found that solid particles, which testing found to be
consistent with heated hydraulic fluid, were found in the hydraulic fluid lines and the connector
port for the right outboard flap actuator. No similar particles were found in any fluid samples
from the airplane’s hydraulic reservoir or from the examined hydraulic system filters. Therefore,
the identified solid particles appeared to have changed state only after exposure to the high
temperatures of the postimpact fire.
The investigation considered that the right inboard flap actuator (installed as original
equipment on the airplane) may have sustained interior damage during the airplane’s 1998 right
engine fire event that may have gone undetected and resulted in a malfunction of the actuator.
The investigation also considered that hydraulic fluid contamination (such as from foreign
particles or air) could result in a flap actuation delay. No evidence of any preexisting condition
was discovered. However, because of the extent of the impact and postcrash fire damage to the
right flaps’ actuators and the hydraulic system components, the investigation could not determine
if any evidence of either condition may have been present before the accident. The NTSB
concludes that, because of the extent of the impact and postaccident fire damage to the right flaps
and flap actuators, the reason for the airplane’s flap asymmetry could not be determined.
The following analysis describes the accident sequence and examines the safety issues
associated with the flight crew’s performance during the approach in response to the flap
anomaly, the dispatch of the flight into freezing drizzle conditions, the communication of flight
crew and HAZMAT information to the emergency response personnel, airplane equipment
considerations, and simulator-based training for pilots who fly in icing conditions.
51

NTSB Aircraft Accident Report
52
2.2 Accident Sequence
During the accident approach, at 0434:24, the first officer was flying using the autopilot
and called for a flap setting of 15°, which is the appropriate approach flap setting for the
ATR 42; however, a flap asymmetry occurred. During a postaccident interview, the first officer
stated that she noticed that the airplane did not decelerate as expected (and briefly accelerated);
however, she did not say anything to the captain about her observation. The airplane’s failure to
decelerate is consistent with a flap asymmetry because the abnormal condition provided less lift
and drag than the desired 15° approach flap configuration. Further, the presence of airframe ice
accretion also affected the drag forces on the airplane. As a result, the engine power settings that
would have been appropriate during a typical approach (with 15° flaps and no ice contamination)
would not have applied to the accident approach. However, the FDR showed that at 0434:54,
about 30 seconds after the asymmetry occurred, the first officer reduced engine power to about
3 percent torque, which was likely an effort to reduce the airspeed; as the airplane continued its
descent on autopilot, only a minimal increase in engine power was commanded.
About 40 seconds after the asymmetry occurred, the captain observed a problem with the
flaps; at this time, the airplane was just outside the LOM/FAF at an altitude of about 1,400 feet
agl. In response, the captain began a nonstandard procedure to troubleshoot the flap problem and
did not verbalize his plan of action with the first officer, who continued flying the approach. The
airplane’s airspeed decreased throughout the approach, resulting in an increasing AOA, and the
stick shaker activated when the airplane was about 900 feet agl at an airspeed of 125 kts. The
airplane performance study found that the stick shaker activated at the setting prescribed for
flight in icing conditions.
93
The stick shaker disconnected the autopilot at 0435:29, and the first officer began to
manually fly the approach, increasing engine power to about 70 percent torque. Control force
estimates showed that the first officer was applying about 35 to 40 lbs of rudder pedal pressure
and about 13 lbs of control wheel force to manually counter the flap asymmetry. However, under
manual control, the airplane deviated high and to the right of the runway 17R ILS glidepath,
indicating that the first officer may not have immediately recognized the extent of the airplane’s
right banking tendency induced by the flap asymmetry. As the deviation increased, at 0435:40,
the first officer asked the captain, “should I go around?” The captain replied, “no” and instructed
the first officer to “keep descending.” About 4 seconds later, when with a strained voice the first
officer stated, “we’re getting close here,” the captain asked the first officer if she wanted him to
take the controls, and she replied that she did.
After the accident, the captain stated that he had not heard the autopilot disconnect alert
and was surprised to see that the first officer was manually flying the airplane. No autopilot
disconnect alert was heard on the CVR. Postaccident testing of the autopilot disconnect alerting
system revealed no malfunctions. On the ATR 42-320, the aural stall warning has priority over
the autopilot disconnect aural alert. By the time that the autopilot disconnect aural alert would
have sounded (about 1.1 seconds after the aural stall warning), the first officer likely responded
93
For more information about the captain’s actions and the flight crew’s training and procedures for responding
to flap anomalies and the stick shaker, see section 2.3.1.

NTSB Aircraft Accident Report
53
to the stall warning by pushing the autopilot disconnect push button, which silenced the pending
autopilot disconnect alert.
When the captain took control, the airplane was about 700 feet agl at 143 KIAS, high and
to the right of the approach course. At 0436:00, about 10 seconds after the captain took control,
the forces exerted on the cockpit controls peaked with maximum forces on the control column,
control wheel, and rudder pedals of 36 lbs, 29 lbs, and 112 lbs, respectively.
94
When these peak
forces were applied, the airplane was descending through about 500 feet agl (the reported
ceiling) and likely emerged from the clouds, allowing the captain to establish visual contact with
the runway. At this time, the airplane was more than 300 feet right of the localizer course, and
the captain’s control inputs were consistent with a course correction to align the airplane with the
runway. About 2 seconds later, the flaps returned to a symmetric state, and control input to
counteract the flap asymmetry was no longer required.
Immediately after the captain exerted the peak forces on the cockpit controls, about
27 seconds before impact, the aural stall warning and the stick shaker activated for the second
time, concurrent with the TAWS warning, “pull up. pull up.” Procedures for responding to either
the stick shaker or the TAWS warning require the immediate application of maximum engine
power; however, 2 seconds later, the captain reduced the airplane’s engine power to about
10 percent torque, and he did not call for maximum engine power until 15 seconds later at
0436:17. As the captain continued the approach, the airspeed again decreased below the
minimum safe approach speed.
At 0436:18, about 9 seconds before impact, the pilot began to pull back on the control
column for several seconds. In response to the pilot’s pull on the control column, the pitch
attitude, AOA, and load factor all began increasing. At 0436:19, the aural stall warning and the
stick shaker activated for the third time. The airspeed when the stall warning occurred was about
124 kts, approximately 19 kts below the minimum safe airspeed for the approach of 143 kts.
About 2 seconds after the stall warning occurred, the airplane experienced an uncommanded roll
followed by a series of roll, yaw, and pitch oscillations, which continued until ground impact.
No evidence existed of airplane performance behavior consistent with an aerodynamic
stall or with a loss of lateral control until after 0436:20. Further, no evidence existed of a sudden
change in aileron hinge movement throughout the approach. The airplane performance study and
simulations determined that the performance degradation due to ice accretion never exceeded the
airplane’s thrust performance, nor would it have exceeded the airplane’s flight control
capabilities if the minimum safe airspeed had been maintained. Therefore, the NTSB concludes
that the airplane was controllable with the flap asymmetry and airframe ice contamination and
could have been maneuvered and landed safely if the minimum safe airspeed had been
maintained.
If the captain had responded appropriately to the concurrent stall and TAWS warnings
that occurred 27 seconds before impact by immediately initiating a go-around maneuver when
the airplane was at an altitude of about 500 feet agl, he likely would have been able to arrest the
94
According to 14 CFR 25.143(d), the maximum control forces allowable for short-term application of pitch
and roll, when two hands are available, and yaw are 75 lbs, 50 lbs, and 150 lbs, respectively.

NTSB Aircraft Accident Report
54
airplane’s descent, increase its airspeed, and avoid an aerodynamic stall. The NTSB concludes
that the captain’s failure to immediately respond to the aural stall warning, the stick shaker, and
the TAWS warning resulted in his inability to arrest the airplane’s descent and avoid impact with
the ground.
2.3 Human Performance
Under normal conditions, the approach-to-landing is a high-workload phase of flight for
pilots. Required tasks include controlling, maneuvering, and configuring the airplane;
performing final landing checks; and evaluating the airplane’s performance relative to the
landing criteria. Pilots are expected to capture and prioritize critical information, analyze that
information, and take appropriate action. Performing these tasks can become increasingly
difficult as workload increases beyond routinely experienced levels, and, during the accident
approach, both the icing conditions and the flap anomaly combined to increase the flight crew’s
workload.
Research demonstrates that emergency situations increase workload and require
additional effort to manage effectively because of the stress involved, human cognitive
limitations, and the lack of opportunity for pilots to practice these skills on a regular basis
compared to the skills used in normal operations.
95
The NASA emergency and abnormal
situations study,
96
which analyzed the NTSB’s findings from its 1994 safety study that reviewed
flight crew-involved, major accidents,
97
also noted that, during high-workload conditions,
performance deficiencies, including narrowing of attention and impairment of short-term
memory, could result from inherent limitations in cognitive processes and the effect of stress on
human performance.
Training, experience, and SOPs are developed to mitigate errors, especially during
dynamic and high-workload situations. However, after the flight crewmembers recognized that a
flap problem existed, they failed to follow their training and did not perform a go-around
maneuver and reference the QRH checklist for the flap anomaly procedure; they did not comply
with Empire Airlines’ procedures (outlined in the GOM) that address abnormal situations. As a
result, a compounding situation unfolded in which the flight crew missed several opportunities to
apply the correct SOPs to ensure the safety of the flight.
SOPs are universally recognized as basic to safe aviation operations. Well-designed cockpit
procedures are an effective countermeasure against operational errors, and disciplined compliance
with SOPs, including strict checklist discipline, provides the basis for effective crew coordination
and performance. Operational data confirm the importance of strict compliance with SOPs for safe
operations.
For example, industry data show that pilots who intentionally deviated from SOPs were
95
R.K. Dismukes, G.E. Young, and R.L. Sumwalt, “Cockpit Interruptions and Distractions: Effective
Management Requires a Careful Balancing Act,” ASRS Directline, vol. 10 (1998), pp 4-9.
96
B.K. Burian, I. Barshi, and K. Dismukes, The Challenge of Aviation Emergency and Abnormal Situations,
NASA Technical Memorandum 2005-213462 (Moffett Field, California: National Aeronautics and Space
Administration, 2005).
97
See A Review of Flight Crew-Involved, Major Accidents of U.S. Air Carriers, 1978 through 1990, Safety
Study NTSB/SS-94/01 (Washington, DC: National Transportation Safety Board, 1994).
NTSB Aircraft Accident Report
55
three times more likely to commit other types of errors, mismanage errors, and find themselves in
undesired situations compared with pilots who did not intentionally deviate from procedures.
98
According to AC 120-71A, in its study of controlled flight into terrain accidents, the Commercial
Aviation Safety Team, which included FAA, industry, and union representatives, found that almost
50 percent of the studied accidents related to the flight crew’s failure to adhere to SOPs or the
certificate holder’s failure to establish adequate SOPs. The NTSB has repeatedly cited casual cockpit
discipline and inadequate compliance with SOPs as contributing factors to accidents.
99
2.3.1 Captain’s Nonstandard Responses
After the captain stated that the airplane had “no flaps,” no further discussion occurred as
to what actions should be taken, and no reference was made to the QRH. Instead, the captain
retrieved and used a flashlight to check the circuit breakers located behind the first officer’s seat
while the first officer continued to fly the approach. During postaccident interviews, the captain
indicated that he checked the circuit breakers because he felt that he needed to determine what
the malfunction was before he could respond with the appropriate checklist. The first officer
stated that she was a little concerned about the captain’s actions and that she thought that he
should have been more focused on the tasks associated with landing the airplane. However, at no
time during the flight did she verbalize her concerns.
Both the captain and the first officer had been trained to perform a go-around maneuver
and reference the QRH if a flap problem occurred during an approach. Based on the flight
crew’s training and the low altitude at which they first noticed the flap anomaly, the appropriate
response would have been to maintain control of the airplane, perform a go-around manuever
(climb the airplane to a safe altitude according to the missed approach procedure), and refer to
the QRH procedure for a flap anomaly. If a go-around maneuver had been performed, after
climbing to 6,000 feet msl, the airplane would have exited icing conditions and reentered a layer
of warmer air with temperatures above freezing. The flight crew could then have completed the
QRH procedure and determined whether to attempt another approach into LBB or proceed to the
flight’s alternate airport, which had no reported precipitation.
Although the captain’s observation that the airplane had “no flaps” was inaccurate
because the airplane actually had a flap asymmetry, the inaccuracy was irrelevant because the
same QRH procedure applied for both a no-flaps condition and a flap asymmetry. The pilots
were trained to verify the flap conditions by looking in the cockpit at the flap position indicator
and out the side windows at the flap position fairings. The procedure would then have been to
98
The data came from the LOSA Collaborative, which is a network of researchers, safety professionals, pilots,
and airline representatives collaborating to provide, among other things, oversight and implementation of line
operational safety audits and a forum of information exchange regarding these audits. More information is available
online at <http://losacollaborative.org/>.
99
For more information, see (a) Collision with Trees and Crash Short of the Runway, Corporate Airlines
Flight 5966, BAE Systems BAE-J3201, N875JX, Kirksville, Missouri, October 19, 2004, Aircraft Accident Report
NTSB/AAR-06/01 (Washington, DC: National Transportation Safety Board, 2006); (b) Attempted Takeoff From
Wrong Runway, Comair Flight 5191, Bombardier CL-600-2B19, N431CA, Lexington, Kentucky, August 27, 2006,
Aircraft Accident Report NTSB/AAR-07/05 (Washington, DC: National Transportation Safety Board, 2007); and
(c) Crash of Pinnacle Airlines Flight 3701, Bombardier CL-600-2B19, N8396A, Jefferson City, Missouri,
October 14, 2004, Aircraft Accident Report NTSB/AAR-07/01 (Washington, DC: National Transportation Safety
Board, 2007).

NTSB Aircraft Accident Report
place the cockpit flap control lever in the position nearest to the actual position of the flaps and
next perform a reduced-flaps landing procedure (in this case, a no-flaps landing). The no-flaps
landing procedure included briefing the no-flaps approach procedure and resetting the airspeed
bugs.
The NTSB acknowledges that recognizing the cockpit warning indicators, identifying the
nature of any problems, and choosing a response procedure requires considerable attention. As
noted beneath the QRH Table of Contents, before a flight crew performs a procedure, the flight
crew “must assess the situation as a whole, taking into consideration the failures, when fully
identified, and the flight constraints imposed.” According to the GOM, in the event of an
inoperative or malfunctioning flight control system, if the airplane is controllable, the flight crew
“should complete only the applicable checklist procedures” and “not attempt any corrective
action beyond those specified.”
Although the NTSB recognizes that the PIC has authority to deviate from prescribed
procedures in the interest of safety, no indication existed that the captain considered this to be an
emergency condition, and the airplane was controllable. Further, the captain identified the flap
anomaly to the extent necessary to select the applicable checklist procedure. The NTSB
concludes that the captain was adequately trained on how to respond to flap anomalies and that
the captain’s statement that the airplane had “no flaps” indicates that he had sufficient
information to recognize that he should immediately perform a go-around maneuver and apply
the appropriate procedure from the QRH that applied to all flap problems.
Both the captain and the first officer had been trained to perform a go-around maneuver
during an approach in which a stick shaker or TAWS warning occurred or an approach that
became unstabilized. Multiple cues existed that indicated the approach was unstabilized,
including excessive deviation from the glidepath (more than 300 feet right at 500 feet agl), sink
rate greater than 1,000 fpm, and airspeed less than the required approach speed. The captain
indicated that he made a judgment call to continue the landing because he was concerned about
the flap anomaly and the icing conditions. However, the captain had extensive experience flying
in icing conditions and was capable of assessing the effects of ice accretion on the airplane’s
performance. Because the airplane had shed ice from its first icing encounter during the descent
into LBB, the captain should have recognized that a climb to 6,000 feet msl would have allowed
the flight to exit icing conditions. Further, the flight crew had selected level 3 ice protection for
the approach, and neither flight crewmember indicated that the ice accretion itself was
worrisome before the flap anomaly occurred. The NTSB concludes that although the captain
indicated that he was concerned about the icing conditions, the presence of airframe ice accretion
within the capabilities of the airplane’s systems does not negate the importance of adhering to
SOPs and performing a go-around maneuver to respond to the multiple cues associated with an
unstabilized approach including excessive deviation from the glidepath, sink rate greater than
1,000 fpm, and airspeed less than the required approach speed. Further, the NTSB concludes
that, had the captain complied with SOPs in response to the flap anomaly, unstabilized approach,
stick shaker, and TAWS warning and initiated a go-around maneuver, the accident likely would
not have occurred.
56
NTSB Aircraft Accident Report
57
2.3.2 Flight Crew’s Failure to Monitor Airspeed
The dynamic nature of the approach phase of flight requires flight crews to monitor
airspeed, and the presence of icing conditions requires an increased awareness of the airspeed
because of the detrimental effects that icing can have on aircraft performance. According to the
ATR 42 pilot handbook, during an ILS approach, the PM is to call out any deviations from
normal altitude, airspeed, or descent rates. The QRH states that, during a non-normal event, the
PF is responsible for the engine power levers, flightpath and airspeed control, aircraft
configuration, and navigation, and the PM is responsible for completing the appropriate checklist
items, actions on the overhead panel, condition levers, and communications.
During the 26 seconds from when the captain identified a flap problem to the first
stick-shaker event, the airplane’s airspeed decreased from about 155 kts (above the red-bug
airspeed of 143 kts for a 0° flap approach in icing conditions) to 125 kts, and the first officer
applied only a minimal adjustment of engine power during this time. As the airspeed decayed,
neither flight crewmember made any verbal reference about airspeed (actual or target), and at no
time did the captain call out the localizer, glideslope, airspeed, or vertical speed deviations.
Each pilot had two indicators available to assist with airspeed monitoring. First, each
pilot had a fixed-scale, moving-pointer analog airspeed indicator. Each airspeed indicator had
four airspeed bugs—yellow, white, red, and internal—that were manually set by each pilot based
on predetermined airspeeds for the flight conditions.
100
The airspeed bugs for approach and
landing in icing conditions should have been set at 121, 123, 143, and 116 kts, respectively. The
captain erroneously briefed the bugs to be set at takeoff speeds in icing conditions, specifically
112, 123, 143, and 106 kts. The captain’s bugs were set at 110, 124, 145, and 109 kts, and the
first officer’s bugs were set at 112, 124, 144, and 106 kts, respectively. Second, a fast/slow
indicator was located on the left side of each pilot’s EADI. The fast/slow indicator alerts the pilot
of the airplane’s actual airspeed in relation to the target airspeed set by the internal bug.
When the pilots realized that a flap anomaly had occurred, the appropriate airspeed to
maintain would have been the red bug, or 143 kts. The crew could have reset the internal bug to
this airspeed to have the additional airspeed cue from the EADI fast/slow indicator, but they did
not do so. Previous accidents
101
have shown that pilots can become distracted from flying duties
when an emergency or abnormal situation occurs, and literature suggests that “one of the biggest
hazards of ‘abnormals’ is becoming distracted from other cockpit duties.”
102
While flying the
100
For more information about the airspeed bugs, see sections 1.6.4.1 and 1.17.1.4.
101
(a) On December 29, 1972, a Lockheed L-1011 crashed when the flight crewmembers failed to monitor their
flight instruments after becoming distracted by a malfunctioning landing gear position indicator, resulting in
101 fatalities. See Eastern Air Lines, Inc., L-1011, N310EA, Miami, Florida, December 29, 1972, Aircraft Accident
Report NTSB/AAR-73/14 (Washington, DC: National Transportation Safety Board, 1973). (b) On June 9, 1995, a
de Havilland DHC-8 crashed when the captain failed to monitor the approach after becoming distracted by first
officer’s attempts to reconcile a landing gear malfunction, resulting in 4 fatalities and 14 serious injuries. See de
Havilland DHC-8, ZK-NEY, Controlled Flight into Terrain, near Palmerston North, 9 June 1995, Investigation
Report 95-011 (Wellington, New Zealand: Transport Accident Investigation Commission, 1997).
<http://www.taic.org.nz> (accessed March 21, 2011). (c) On April 19, 2008, a Cessna 510 overshot the runway
during landing in Carlsbad, California, after the pilot became distracted by a flickering primary flight display and
misjudged the airspeed and landing distance. The report for this accident, NTSB case number LAX08FA117, is
available online at <http://www.ntsb.gov/aviationquery/index.aspx>.
102
Dismukes, Young, and Sumwalt, pp 4-9.

NTSB Aircraft Accident Report
approach, the first officer was likely distracted from monitoring the instruments by the flap
anomaly, the captain’s nonstandard actions involving the circuit breakers, and the control force
inputs needed to maintain control of the airplane because of the flap asymmetry. Further, for the
captain to check circuit breakers behind the first officer’s seat, he would need to turn away from
the instrument panel, a position from which monitoring the instruments was not possible. The
NTSB concludes that the first officer’s failure to maintain airspeed while acting as the PF likely
resulted from being distracted by the flap anomaly, the captain’s actions in response to it, and the
control force inputs needed to maintain aircraft control. Further, the NTSB concludes that the
captain’s failure to call out the first officer’s airspeed deviations resulted directly from his
preoccupation with performing an inappropriate, nonstandard procedure in response to the flap
anomaly.
2.3.2.1 Airspeed References
As previously mentioned, the airspeed bugs were not set properly because the captain did
not correctly brief the airspeeds for an approach in icing conditions; instead, he erroneously
briefed the airspeeds for a takeoff in icing conditions. It is not clear why neither crewmember
recognized the captain’s error; however, at the time of the accident, Empire Airlines did not have
a procedure in place for flight crews to crosscheck and verify the setting of airspeed bugs.
Empire Airlines has since implemented a crosscheck procedure. Also, because the captain did
not perform the QRH procedure after identifying the flap anomaly, he did not brief the new
approach speeds, and the flight crew did not reset the airspeed bugs accordingly.
Because the flight crew failed to properly set the internal airspeed bug, the EADI
fast/slow indicator, which indicates the difference between the internal bug airspeed and the
airplane’s actual airspeed, provided indications that did not apply to the accident approach.
However, the captain had correctly stated during his initial briefing that the airspeed for the red
bug, which indicates the approach airspeed for 0° flaps in icing conditions, was 143 kts, and both
red bugs were set near that value (144 and 145 kts). Therefore, the NTSB concludes that,
although some of the airspeed bugs (including the internal bug) were not set to the appropriate
approach airspeeds and were not reset following recognition of the flap anomaly, the flight crew
had a sufficient reference to maintain the minimum safe airspeed because the airspeed for a
no-flap approach in icing conditions was correctly briefed as 143 kts, and the red airspeed bugs
were set near that value.
The airspeed indicator is a visual cue that can convey meaning to flight crewmembers
only when they look at the indicator. As discussed previously, the first officer was distracted
from monitoring the visual airspeed indications, and the captain’s attention was focused away
from the instrument panel. Evidence from this accident and others indicates that, in
high-workload situations, a visual-only cue may not capture a pilot’s attention due to human
sensory limitations.
The airplane’s stall protection system, which included an aural warning and tactile stick
shaker, is designed to comply with Federal airworthiness standards, specifically
58

NTSB Aircraft Accident Report
59
14 CFR 25.207,
103
that require airplanes be equipped to provide flight crews with a clear and
distinctive stall warning at an airspeed that is about 7 percent higher than stall airspeed. When
the flight crew became distracted by the flap anomaly and failed to detect that the airplane was
approaching a stall, the stall protection system activated as designed and warned the flight crew
of the decaying airspeed. However, the airspeed began to decay unnoticed much earlier during
the approach. The airspeed indicator should have provided the pilots with adequate time to detect
the ensuing low-airspeed regime and respond appropriately. However, distraction and workload
considerations may have made it difficult for the flight crew to visually detect these cues. The
NTSB concludes that reliance upon flight crew vigilance and stall warning systems may be
inadequate to prevent hazardous low-airspeed situations and that, had a low-airspeed alerting
system been installed on the airplane, it may have directed the flight crew’s attention to the
decaying airspeed earlier and provided an opportunity to take corrective action before the stall
protection system activated.
The circumstances of this accident and the history of accidents involving flight crews’
lack of low-airspeed awareness, most recently the flight crew of Colgan Air flight 3407,
104
suggest that flight crew vigilance and existing stall warnings may be inadequate to reliably
prevent hazardous low-airspeed situations. In the Colgan Air accident, the pilots likely did not
see the rising low-airspeed cue on the indicated airspeed display, the downward-pointing trend
vector, or the airspeed indications change to red. As a result, the NTSB concluded that an aural
warning in advance of the stick shaker would have provided a redundant cue of the visual
indication of the rising low-airspeed cue and might have elicited a timely response from the
pilots before the onset of the stick shaker. Therefore, the NTSB issued Safety Recommendation
A-10-12,
105
which recommended that, for all airplanes engaged in commercial operations under
14 CFR Parts 121, 135, and 91 subpart K, the FAA require the installation of low-airspeed
alerting systems that provide pilots with redundant aural and visual warnings of an impending
hazardous low-airspeed condition. Because of the FAA’s inactivity regarding previous
recommendations to require the installation of low-airspeed alerting systems, the NTSB
classified Safety Recommendation A-10-12 “Open—Unacceptable Response” when it was
issued on February 23, 2010.
Although the FAA has tasked the ARAC with developing recommendations for potential
requirements to address low-airspeed alerting systems, progress remains slow, and the
recommendation is still classified “Open—Unacceptable Response.” This accident once again
103
At the time the ATR 42 was certificated in 1988, 14 CFR 25.207(c) stated that “the stall warning must begin
at a speed exceeding the stalling speed (i.e., the speed at which the airplane stalls or the minimum speed
demonstrated, whichever is applicable under the provisions of 14 CFR 25.201(d)) by seven percent or at any lesser
margin if the stall warning has enough clarity, duration, distinctiveness, or similar properties.” The current version
of 14 CFR 25.207(c) states that “when the speed is reduced at rates not exceeding one knot per second, stall warning
must begin, in each normal configuration, at a speed, V
SW
, exceeding the speed at which the stall is identified in
accordance with 14 CFR 25.201(d) by not less than five knots or five percent CAS, whichever is greater. Once
initiated, stall warning must continue until the angle of attack is reduced to approximately that at which stall warning
began.”
104
NTSB/AAR-10-01.
105
For more information about Safety Recommendation A-10-12, see section 1.18.2.3.

NTSB Aircraft Accident Report
60
demonstrates the need for low-airspeed alerting systems and provides additional support for this
recommendation.
106
2.3.2.2 Flight Crew Monitoring Skills and Techniques
The accident flight crew’s deficiencies during the approach demonstrate the importance
of active monitoring skills. However, the flight crew’s CRM training did not specifically address
the development of active monitoring skills.
107
The NTSB has long recognized the importance of
flight crew monitoring skills in accident prevention. In 1994, the NTSB published a safety
study
108
that reviewed 37 flight crew-related, major accidents involving U.S. air carriers and
found that, for 31 of these accidents, inadequate monitoring and/or crosschecking had occurred.
The safety study found that flight crewmembers frequently failed to recognize and effectively
draw attention to critical cues that led to the accident sequence.
As a result of this safety study, the NTSB issued safety recommendations that resulted in
upgrades of FAA training guidance, including revisions to AC 120-51B (currently AC 120-51E),
“Crew Resource Management Training,” and AC 120-71 (currently AC 120-71A), “Standard
Operating Procedures for Flight Deck Crewmembers,” to include references to the importance of
flight crew monitoring functions. Subsequently, the NTSB issued Safety Recommendation
A-07-13,
109
which asked the FAA to require that all pilot training programs contain modules that
teach and emphasize monitoring skills and workload management and include opportunities to
practice and demonstrate proficiency in these areas.
On May 17, 2007, the FAA stated that it would consider identifying in its work program
a list of required inspections, reemphasizing to the regional and FSDO managers the need to
validate the training and to verify its effectiveness. However, the FAA’s lack of progress in this
area and the February 12, 2009, Colgan Air accident
110
in which the flight crew failed to monitor
airspeed prompted the NTSB to reiterate Safety Recommendation A-07-13 and reclassify it
“Open—Unacceptable Response” on February 23, 2010. On the same date, the NTSB issued
Safety Recommendation A-10-10,
111
which asked the FAA to require 14 CFR Part 121, 135, and
91 subpart K operators to review their SOPs to verify that they are consistent with the flight crew
monitoring techniques, as described in AC 120-71A. On June 22, 2010, the FAA responded that
it was considering issuing a SAFO or an InFO bulletin to address this recommendation. On
January 25, 2011, the NTSB indicated that, although such action may represent part of an
acceptable response to this recommendation, the FAA must also ensure that the guidance
provided in documents like SAFOs is implemented. This accident again demonstrates the
importance of flight crew monitoring skills in accident prevention and provides additional
support for Safety Recommendations A-07-13 and A-10-10.
106
For information about ATR’s APM technology that provides icing-specific airspeed alerts, see section 2.6.1.
107
For information about other CRM topics, see section 2.3.3.
108
NTSB/SS-94/01.
109
For more information about Safety Recommendation A-07-13, see section 1.18.2.1.
110
NTSB/AAR-10/01.
111
For more information about Safety Recommendation A-10-10, see section 1.18.2.1.

NTSB Aircraft Accident Report
61
2.3.3 Crew Resource Management
During the accident flight’s initial descent, the flight crew demonstrated several instances
of good CRM; the captain completed the descent checklist and immediately began the approach
checklist in anticipation of the first officer’s needs. However, after the flap anomaly was
recognized, the flight crew’s CRM deteriorated to the extent that the captain did not provide
adequate leadership in response to the anomaly. Further, the first officer was not assertive in
voicing her concerns about the captain’s nonstandard response or his decision to continue the
unstabilized approach. The captain is responsible for setting the tone in the cockpit for the entire
flight, and this responsibility was even more critical because the flight crew was faced with an
abnormal situation.
The accident captain had about 13,935 total flight hours (2,052 hours of which were in
the ATR 42) and extensive experience flying in icing conditions. He had previously served as a
check airman on the company’s single-pilot Cessna 208 airplanes. The first officer had about
2,109 total flight hours (130 hours of which were as SIC in the ATR 42) and very limited
experience flying in icing conditions. The captain had been with Empire Airlines for more than
20 years.Thus, he should have been very familiar with the company’s SOPs, and the accident
flight crew should have been able to benefit from the captain’s extensive experience with the
company, in ATR 42 airplanes, and with flying in icing conditions. However, the captain failed
to command control of the situation and follow SOPs. Following identification of the flap
anomaly, the captain did not communicate to the first officer his intentions for managing the
situation. Instead, the captain pursued his own plan of action without providing any guidance to
the first officer or performing the duties required of him as the PM, which could have helped the
first officer manage the airplane during the approach.
The large disparity between the captain’s and the first officer’s flying experience, their
experience in the ATR 42, and their experience in icing conditions likely created a steep
authority gradient in the cockpit. The flight crewmembers who flew with the captain stated in
interviews that, overall, he was very experienced, a good pilot, and a good captain. He was
referred to as a “guru.” The issue of cockpit authority gradient has been examined since the late
1970s and has been evident in a number of major aviation accidents, including the March 27,
1977, collision of two Boeing 747s at Tenerife Airport, Los Rodeos, Spain.
112
Evidence has
suggested that too steep of a gradient can reduce flight crew performance, hinder
communication, and increase errors. For example, a review of U.S. Navy mishaps between 1980
and 1990 revealed that flight crews with an authority gradient of one rank or more between flight
crewmembers had 21 percent more errors than flight crews in which the crewmembers were of
the same rank.
113
In a study of 249 airline pilots in the United Kingdom, nearly 40 percent of
first officers stated that they failed to communicate safety concerns to their captains on more
112
See KLM B-747, PH-BUF, and Pan Am B-747, N736PA, Collision at Tenerife Airport, Los Rodeos, Spain,
on 27 March 1977, Aircraft Accident Report (Spain: Subsecretaría de Aviación Civil, 1978).
113
R.A. Alkov and others, “The Effect of Trans-Cockpit Authority Gradient on Navy/Marine Helicopter
Mishaps,” Aviation, Space, and Environmental Medicine, vol. 63, no. 8 (1992), pp. 659-661.

NTSB Aircraft Accident Report
62
than one occasion for reasons that included a desire to avoid conflict and deference to the
captain’s experience and authority.
114
The poor CRM observed in this accident is similar to that which the NTSB found during
its investigation of the February 19, 1996, crash of Continental Airlines flight 1943 in Houston,
Texas.
115
During the event sequence leading to the accident, the captain rejected, without any
discussion, the first officer’s go-around request, and the first officer failed to challenge his
decision. The flight crew failed to complete multiple checklists and continued an unstabilized
approach below 500 feet
116
against company procedures to go around in such situations. As a
result of this accident, the NTSB issued Safety Recommendations A-97-05 and -06,
117
which
asked the FAA to require all POIs of 14 CFR Part 121 carriers to 1) ensure that the carriers
establish a policy and make it clear to their pilots that there will be no negative repercussions for
appropriate questioning in accordance with CRM techniques of another pilot’s decision or action
and 2) ensure that CRM programs provide pilots with training in recognizing the need for, and
practice in presenting, clear and unambiguous communications of flight-related concerns.
On October 30, 1998, the FAA issued AC 120-51C (currently AC 120-51E), which
emphasized the importance of all levels of management to support a safety culture that promotes
communication by encouraging appropriate questioning and that there will be no negative
repercussions for appropriate questioning of one pilot’s decision or action by another. Based on
the FAA’s lack of action to issue an FSIB, on February 23, 2000, the NTSB classified these
recommendations “Closed—Unacceptable Action.” Thirteen years after the FAA issued
AC 120-51C, the NTSB continues to investigate accidents in which one pilot does not question
the actions or decisions of another pilot.
To overcome large authority gradients, AC 120-51E suggests that assertiveness be
included in CRM training programs. FlightSafety’s CRM training materials for Empire Airlines’
flight crewmembers included two presentation slides that encouraged pilots to speak up with
“appropriate persistence until there is a clear resolution.” However, the accident first officer
could not recall what was trained during the 2-day CRM training course, including whether or
not assertiveness was addressed.
According to Empire Airlines’ ATR 42 pilot handbook, if a go-around maneuver is
required, the PF should call out “go around” and initiate the go-around procedures. During the
accident flight, the first officer instead asked the captain, “should I go around?,” rather than
directly asserting her concern about the unstabilized approach, even though she was aware that
company policy was to go around in the event of stick-shaker activation. The first officer
indicated that asking was her way of saying that she wanted to go around “without stepping on
toes.” Captains who had previously flown with the first officer stated that, although she did not
seem to have a problem standing up for something in the cockpit, she asked a lot of questions
when flying that were related to skills that she already knew.
114
J. Wheale, “Crew Coordination on the Flight Deck of Commercial Transport Aircraft,” Proceedings of the
Flight Operations Symposium, October 1983 (Dublin: Irish Air Line Pilots Association/Aer Lingus, 1983).
115
NTSB/AAR-97/01.
116
A ground proximity warning system alert continued below 200 feet above field elevation.
117
For more information about Safety Recommendations A-97-05 and -06, see section 1.18.2.4.

NTSB Aircraft Accident Report
63
The first officer stated that, after the captain responded “no” to her go-around inquiry, she
felt that he had a good reason for not wanting to go around and that she trusted that he was
making the right decisions. The first officer stated that, after the captain took control of the
airplane, she was still concerned with the approach and felt that she should have called again for
a go-around maneuver but that she did not know why she did not say anything. The NTSB
concludes that the first officer’s failure to assert herself to the captain and initiate a go-around
maneuver when she recognized the unstabilized approach likely resulted from the steep authority
gradient in the cockpit and the first officer’s minimal training on assertiveness; further, the
captain’s quick dismissal of the first officer’s go-around inquiry likely discouraged the first
officer from voicing her continued concerns and challenging the captain’s decision to continue
the unstabilized approach. The NTSB notes that the first officer’s CRM training did not include
any role-playing activities in which pilots could practice developing assertiveness skills. Practice
allows pilots to bridge the gap between their knowledge of assertiveness and the actions needed
in the cockpit to effectively be assertive.
118
The NTSB concludes that role-playing exercises are
essential for effective assertiveness training because such exercises provide flight crews with
opportunities for targeted practice of specific behaviors and feedback that a lecture-based
presentation format lacks. Therefore, the NTSB recommends that the FAA require that
role-playing or simulator-based exercises that teach first officers to assertively voice their
concerns and that teach captains to develop a leadership style that supports first officer
assertiveness be included as part of the already required CRM training for 14 CFR Part 121, 135,
and 91 subpart K pilots.
2.3.4 Go-Around Callout
Empire Airlines’ ATR 42 pilot handbook specified that the phrase “go around” is to be
stated out loud by the PF; however, the operating procedures did not provide any guidance
indicating that the PM could initiate the same action. Similarly, Empire Airlines’ flight training
materials contained no guidance that indicated whether either pilot could call for a go-around
maneuver, if necessary.
During the NTSB’s investigation of the February 18, 2007, Shuttle America runway
overrun accident,
119
the NTSB noted that it is critical to flight safety that either flight
crewmember be able to call for a go-around maneuver if either pilot believes that a landing
would be unsafe. As a result, the NTSB issued Safety Recommendation A-08-18,
120
which asked
the FAA to require operators to have a written policy emphasizing that either pilot can make a
go-around callout and that the proper response to such a callout is an immediate missed
approach. On March 1, 2010, the FAA issued SAFO 10005, “Go-Around Callout and Immediate
Response,” which recommended that operators provide such a written policy. However, the FAA
has not yet revised FAA Order 8900.1 to include guidance to POIs to have operators develop the
written policy and has not yet completed a survey to ensure that all operators have developed and
118
R.L. Beard, E. Salas, and C. Prince, “Enhancing Transfer of Training: Using Role Play to Foster Teamwork
in the Cockpit,” International Journal of Aviation Psychology, vol. 5, no. 2 (1995), pp. 131-143.
119
NTSB/AAR-08/01.
120
For more information about Safety Recommendation A-08-18, see section 1.18.2.2.
NTSB Aircraft Accident Report
64
implemented this policy. The NTSB encourages the FAA to take timely action in response to this
recommendation.
2.3.5 Training for Single and Multiple Abnormal Situations Occurring at Low
Altitude
As this accident shows, pilots can encounter rapidly changing conditions during
approach-to-landing operations. The accident flight crew encountered a flap asymmetry while
operating in moderate icing conditions. (Moderate icing conditions, although considered a
normal situation in the AFM, increase flight crew workload.) Because any distraction from
maintaining airplane controllability at low altitude can lead to dire consequences, pilots must be
familiarized with the rapid decision-making and maneuvering skills required to ensure safe
flight, especially when operating near the ground. During the accident flight, the captain
remained committed to continuing the approach, even though he was trained that (and SOPs
required that) a go-around maneuver should be performed and even after he received multiple
indications that the approach had become dangerously unstabilized.
After the accident, the captain explained that he “just wanted to land as soon as possible.”
The 1998 NASA study
121
found that the most common decision errors occurred when the flight
crew decided to “continue with the original plan of action in the face of cues that suggested
changing the course of action.” The NASA study stated that the cues that signal a problem are
not always clear and that a decision maker’s assessment of the situation may not keep pace with
conditions that deteriorate gradually. The NASA study also indicated that individuals have a
natural tendency to maintain their originally selected course of action until clear and
overwhelming evidence exists that the course of action should be changed. In addition, the study
noted that pilots under stress might not evaluate the consequences of various options.
On May 19, 2009, as a result of the NTSB’s investigation of the September 28, 2007,
American Airlines flight 1400 accident,
122
which involved multiple, simultaneous abnormal
situations, the NTSB issued Safety Recommendations A-09-24 and -25,
123
which asked the FAA
to establish best practices for conducting both single and multiple emergency and abnormal
situations training and to require that these best practices be incorporated into all operators’
approved training programs. Although the FAA has made progress by publishing its January 12,
2009, NPRM, “Qualification, Service, and Use of Crewmembers and Aircraft Dispatchers,”
124
which included scenario-based training for all 14 CFR Part 121 carriers, the NTSB is concerned
that, without a guide to best practices, inspectors and operators will have difficulty creating
effective programs. The FAA has not yet completed a review of the regulatory and policy
framework to determine whether additional guidance or requirements are necessary.
121
J. Orasanu, L. Martin, and J. Davison, Errors in Aviation Decision Making: Bad Decisions or Bad Luck?,
NASA Ames Research Center, Moffett Field, California. Presented to the Fourth Conference on Naturalistic
Decision Making, Warrenton, Virginia, May 29-31, 1998.
122
NTSB/AAR-09/03.
123
For more information about Safety Recommendations A-09-24 and -25, see section 1.18.2.1.
124
74 FR 1280. (The FAA subsequently began work on an NPRM supplement, which was submitted to the
Office of Management and Budget (OMB) for review on November 29, 2010.
As of the date of this report, OMB is
continuing to review this supplemental NPRM with no projected completion date.)

NTSB Aircraft Accident Report
65
The NTSB recognizes that operators have limited time to allocate to training. However,
this accident and others show that pilots could benefit from opportunities to develop the skills
and decision-making abilities needed during single and multiple abnormal situations; such
training can present pilots with competing task demands and increased workloads and can
demonstrate in a safe environment the possible consequences of not taking timely, appropriate
corrective action. This accident illustrates that these skills are most important at low altitudes
when rapid, accurate assessment of abnormal situations and appropriate prioritization of tasks are
the most critical. Thus, the NTSB concludes that the establishment of best practices for
conducting both single and multiple emergency and abnormal situations training needs to include
training for the occurrence of these situations at low altitudes because low-altitude scenarios
require rapid, accurate assessment of abnormal situations and appropriate prioritization of tasks.
The circumstances of this accident reinforce the need for the actions recommended in Safety
Recommendations A-09-24 and -25, and the NTSB encourages the FAA to take timely action in
response to these recommendations.
2.3.6 Fatigue Considerations
The NTSB evaluated a number of criteria
125
to determine the extent to which fatigue
impacted the flight crew’s performance during the accident sequence including circadian factors,
sleep length, and time awake.
The accident occurred about 0437, and the flight crewmembers were awake in opposition
of their normal circadian rhythm. For those entrained on a diurnal schedule, the primary
circadian trough is about midnight to 0600, with the window of circadian low generally
occurring between about 0300 and 0500. The aeromedical research community has identified
strategies that flight crews can use to lessen the adverse effects of fatigue during required
overnight operations. These strategies include avoiding morning sunlight and staying indoors,
ensuring the daytime sleep environment is dark and cool, wearing eye masks and earplugs during
daytime sleep, implementing good sleep habits, taking a short nap before reporting for duty,
allowing exposure to at least 2 hours of sunlight or bright artificial light in the late afternoon or
early evening after waking, strategically using caffeine, and getting regular exercise.
126
Both
flight crewmembers took some actions before the accident to reduce the likelihood of
performance decrements associated with being awake during the nighttime hours.
For example, during the week before the accident flight (January 20 through 23), the first
officer had a scheduled trip in which she was on duty during the night hours beginning about
0045. She was off duty from the afternoon of January 23 through the evening of January 26.
Empire Airlines paid her expenses to spend the weekend in Midland, Texas, rather than
commuting back to her home in Washington for a short turnaround.
127
The first officer stated
125
Information regarding the NTSB’s methodology for investigating operator fatigue is available online at
<http://www.ntsb.gov/info/fatigue_checklist_V%202_0.pdf>.
126
M. Caldwell and others, “Fatigue Countermeasures in Aviation,” Aviation, Space, and Environmental
Medicine, vol. 80, no. 1 (2009), pp. 29-59.
127
The flight crew was based in Salt Lake City, which was considered to be a “floater” base. The flight
crewmembers would travel to various cities based on the needs of the company, which paid their expenses over the
weekend.
NTSB Aircraft Accident Report
66
that because she had acclimated herself to sleeping during the days and being awake at night for
the previous trip, she remained on that sleep/wake schedule during her off-duty days rather than
resetting her circadian rhythm to a diurnal pattern of being awake during the day and sleeping at
night. During the 3 days before the accident, the first officer indicated that she went to bed about
0600 and awoke between about 1400 and 1500, providing a sleep opportunity each night of
between 8 and 9 hours.
128
Based on these times, the first officer went to bed before sunrise, thus
avoiding morning sunlight, and awoke before sunset, allowing exposure to bright daylight before
reporting for duty, which would have contributed to her ability to shift her circadian clock.
129
Research suggests that adjustment to night activity is possible, and, under ideal conditions, the
adjustment occurs about 1 hour per day.
130
However, a NASA study examining pilots in
overnight cargo operations found that the circadian clock of pilots did not shift completely as
measured by temperature minimums;
131
the circadian low was delayed about 3 hours after 5 days
of night flying.
132
Although the first officer’s efforts to adapt to an overnight schedule suggest an
individual awareness of the need to mitigate fatigue hazards associated with overnight
operations, and the first officer was possibly able to delay her window of circadian low to some
degree, it is unlikely, based on the available research data, that her efforts would have completely
mitigated the circadian effects of fatigue associated with the time at which the accident occurred.
Sleep needs vary by individual. In postaccident interviews, the first officer stated that she
needed 7 hours of sleep to feel rested. In the 72 hours before the accident, she had 25.5 hours of
sleep opportunity (8.5 hours, 8 hours, and 9 hours in the previous three nights). She indicated
that she felt rested on the evening of the accident. The first officer’s sleep schedule during her
previous trip is unknown. The NASA study examining pilots in overnight cargo operations found
that, while on duty, 54 percent slept over 1 hour less per 24 hours than they did on pre-trip days,
29 percent slept over 2 hours less per 24 hours than they did on pre-trip days, and 15 percent
averaged more sleep per 24 hours than they did on pre-duty days.
133
Post-duty days allowed
pilots to recuperate some of their lost sleep. Specifically, the pilots in the study slept 41 minutes
longer per 24 hours during post-duty days than pre-trip days and 1.9 hours longer per 24 hours
during post-duty days than duty days. Although the first officer had sleep opportunities in excess
of the hours of sleep she needed to feel rested during her off-duty days and had the opportunity
to recuperate any sleep debt accrued, it is unknown as to how much sleep she actually received.
Therefore, it cannot be determined whether the first officer had accumulated a sleep debt during
the week before the accident.
128
The first officer stated that she needed 7 hours of sleep per night to feel rested.
129
Night conditions would have prevailed at the time of the first officer’s reported bedtime, which was more
than 1 hour before sunrise in Midland, Texas. For the week before the accident, sunrise ranged from about 0745 to
0748, and sunset ranged from about 1810 to 1817.
130
R. Wever, “Phase Shifts of Circadian Rhythms due to Shifts of Artificial Zeitgebers,” Chronobiologia,
vol. 7 (1980), pp. 303-327.
131
Core body temperature minimums typically occur in the circadian trough and can be associated with sleep
tendency. Caldwell and others, p. 42.
132
P.H. Gander and others, “Flight Crew Fatigue IV: Overnight Cargo Operations,” Aviation, Space, and
Environmental Medicine, vol. 69, no. 9 (1998), pp. B26-B36.
133
Gander and others, pp. B28-B29.
NTSB Aircraft Accident Report
67
At the time of the accident, the first officer had been awake about 13.5 hours. Research
into quantifying performance impairment associated with sustained wakefulness found that
performance remains relatively stable throughout the time that coincides with a normal waking
day, but that prolonged wakefulness of 17 hours can result in measurable performance
impairment (comparable to having a blood alcohol concentration of 0.05 percent).
134
The first
officer did not have such prolonged or otherwise excessive periods of wakefulness before the
accident.
The captain also took steps to minimize the effects of fatigue due to the circadian clock.
On the night before the accident trip, the captain went to sleep about 2200 but, to prepare himself
for the upcoming night flight, awoke about 0400 on January 26, 2009. Later that afternoon, he
napped from about 1100 to 1630, providing a 5.5-hour sleep opportunity. The captain stated that
he needed 6 to 8 hours of sleep each night to feel rested. In the 72 hours before the accident, the
captain had 22 hours of sleep opportunity (10 hours, 6 hours, and 5.5 hours). The captain stated
that he felt rested on the evening of the accident. Although research suggests that appropriately
placed naps can improve alertness for up to 24 hours,
135
because the accident occurred during the
window of circadian low, the captain was likely experiencing some fatigue at the time of the
accident. In addition, if the captain required 8 hours of sleep per night to feel rested, he may have
been experiencing as much as 4.5 hours of cumulative sleep loss on the night of the accident.
Research suggests that as few as 2 hours of sleep loss can lead to reduced performance and
alertness.
136
At the time of the accident, the captain had been awake about 12 hours, which
would not be considered excessive.
2.3.6.1 Role of Fatigue in Flight Crew Performance
The negative effects of fatigue on human performance have been demonstrated in
scientific research and accident and incident investigations.
137
These effects include slowed
response time, reduced vigilance, and poor decision making. The flight crew’s failure to monitor
134
(a) D. Dawson and K. Reid, “Fatigue, Alcohol and Performance Impairment,” Nature, vol. 388, no. 6639
(1997), p. 235. (b) N. Lamond and D. Dawson, “Quantifying the Performance Impairment Associated with
Sustained Wakefulness” (Woodville, South Australia: The Centre for Sleep Research, The Queen Elizabeth
Hospital, 1998). <http://cf.alpa.org/internet/projects/ftdt/backgr/Daw_Lam.html> (accessed March 21, 2011).
135
D.F. Dinges and others, “Temporal Placement of a Nap for Alertness: Contributions of Circadian Phase and
Prior Wakefulness,” Sleep, vol. 10, no. 4 (1987), pp. 313-329.
136
R. T. Carskadon, “Sleep Restriction,” ed., Sleep, Sleepiness and Performance, T. H. Monk, ed. (Chichester,
England: John Wiley & Sons, 1991), pp. 155–167.
137
For the scientific research, see J.A. Caldwell, “Fatigue in the Aviation Environment: An Overview of the
Causes and Effects as Well as Recommended Countermeasures,” Aviation, Space, and Environmental Medicine,
vol. 68 (1997), pp 932-938; G.P. Kruger, “Sustained Work, Fatigue, Sleep Loss, and Performance: A Review of the
Issues,” Work and Stress, vol. 3 (1989), pp 129-141; and F.H. Previc and others, “The Effects of Sleep Deprivation
on Flight Performance, Instrument Scanning, and Physiological Arousal in Pilots,” The International Journal of
Aviation Psychology, vol. 19, no. 4 (2009), pp. 326-346. For the accident investigations, see, for example, Crash
During Attempted Go-Around After Landing East Coast Jets Flight 81 Hawker Beechcraft Corporation 125-800A,
N818MV Owatonna, Minnesota July 31, 2008, Aircraft Accident Report NTSB/AAR-11/01 (Washington, DC:
National Transportation Safety Board, 2011). <http://www.ntsb.gov/Publictn/2011/AAR-11-01.pdf>; Collision with
Trees and Crash Short of Runway, Corporate Airlines Flight 5966, British Aerospace BAE-J3201, N875JX,
Kirksville, Missouri, October 19, 2004, Aircraft Accident Report NTSB/AAR-06/01 (Washington, DC: National
Transportation Safety Board, 2006). <http://www.ntsb.gov/publictn/2006/AAR0601.pdf>.

NTSB Aircraft Accident Report
the airplane’s airspeed following the flap anomaly could be consistent with the known effects of
fatigue; however, this type of error has also been made by flight crews who were not fatigued.
Throughout the flight, the first officer demonstrated good performance, including
correcting the captain when setting up the approach, questioning the meaning of the Mu readings
provided by ATC, and identifying the need to execute a go-around maneuver after the stall
warning activated. Her failure to monitor airspeed and maintain a stabilized approach did not
occur until after the flap anomaly, while the captain was performing a nonstandard
troubleshooting procedure. The first officer queried the captain as to whether she should go
around, and he told her “no.” The first officer was flying an airplane in which she had little
experience and in conditions that she had never before experienced. As a result, the first officer
relied on the captain’s leadership and experience for guidance, and his instructions to continue
the unstabilized approach contradicted SOPs and likely contributed to her failure to assert her
concerns further. In addition, the captain failed to delegate duties in the abnormal situation, and
his nonstandard approach to address the flap anomaly likely distracted her from her PF duties.
The NTSB concludes that, although the risk for fatigue existed at the time of the accident due to
the window of circadian low, the first officer took steps to mitigate the effects of fatigue, and her
errors during the flight can be explained by her lack of experience in both the airplane and in
icing conditions along with the distraction caused by the captain’s nonstandard response to the
flap anomaly.
Unlike the first officer, the captain made a number of errors throughout the flight,
including briefing the incorrect approach airspeeds, failing to monitor the first officer’s
approach, and performing a nonstandard and nontrained procedure in response to the flap
anomaly. The captain’s decision not to follow SOPs for checklist usage and the unstabilized
approach might be explained through his actions demonstrated on previous flights (another pilot
had indicated that the captain occasionally cut corners, seemed rushed, and was less thorough on
briefings than other captains) and the stress associated with the situation. However, the captain’s
repeated errors and decision to forego procedures might also reflect degradation from fatigue as a
result of performing during a time when he was normally asleep, as well as performing with a
sleep debt. The NTSB concludes that, due to the early morning hour of the accident flight and
the captain’s cumulative sleep debt, fatigue likely degraded the captain’s performance. The
NTSB notes that careful adherence to SOPs, including strict adherence to accepted practices of
stabilized approach criteria, non-normal procedures, and CRM, can help flight crews mitigate the
degrading effects of fatigue. The NTSB further notes that neither the captain nor the first officer
received specific training from their company addressing the hazards of fatigue or fatigue
mitigation, although fatigue was briefly addressed during CRM training.
On September 10, 2010, the FAA addressed some aspects of fatigue by issuing an NPRM
titled “14 CFR Parts 117 and 121: Flightcrew Member Duty and Rest Requirements,” which
proposes to amend Part 121 and establish Part 117 to create a single set of flight time limitations,
duty period limits, and rest requirements for Part 121 operations. The NPRM also proposes
requiring a fatigue education and training program for all flight crewmembers, employees
involved in operational control and scheduling of flight crewmembers, and personnel having
management oversight of these areas. The FAA is currently drafting AC 120-FT, “Fatigue
Training,” that will present guidelines for developing and implementing a fatigue training
program. The draft guidance outlines a training program that includes, in part, a review of the
68
NTSB Aircraft Accident Report
69
basics of fatigue, including an overview of circadian rhythms, the causes of fatigue, the effect of
fatigue on performance, fatigue countermeasures and mitigation, and lifestyle influences on
fatigue.
On November 15, 2010, the NTSB commented on the NPRM and stated, “if adopted, the
proposed rule will provide substantial benefits towards reducing the hazards associated with
flight crew fatigue in Part 121 operations.” The NTSB also stated its strong support for the
requirement of a fatigue education and training program, noting that fatigue education is among
the foundational elements of an effective fatigue management system.
The NTSB is encouraged by the FAA’s response to fatigue mitigation for Part 121
operations based on the NPRM. In recent years, a number of accidents involving Part 121
operators have occurred in which fatigue was causal, contributory, or identified as a safety issue.
The NTSB believes that finalizing the rule in a timely fashion will provide substantial benefits
towards reducing the hazards associated with flight crew fatigue in Part 121 operations and is
critical to aviation safety.
2.4 Operations Issues
2.4.1 Dispatch into Freezing Drizzle Conditions
The flight release for the accident flight contained weather information that indicated that
IFR conditions with light freezing drizzle and mist were reported at LBB and that such
conditions were forecast to continue beyond the flight’s estimated time of arrival. During the
flight’s descent toward LBB, the controller informed the flight crew that light freezing drizzle
and mist were reported at the airport.
Although SLD conditions like freezing rain or freezing drizzle are outside the ATR 42’s
certification icing envelope as specified in 14 CFR Part 25, Appendix C, the FAA does not
specifically prohibit operators from dispatching or operating airplanes in such weather
conditions. Instead, the FAA requires that operators adhere to any AFM limitations for the
airplanes that they operate. The NTSB has long been concerned about such operations and issued
numerous safety recommendations in the 1980s
138
and the 1990s
139
related to the issue. In
response to these recommendations, the FAA issued an NPRM.
140
For the ATR 42, the AFM states that a flight crew must immediately exit severe icing
conditions when they are encountered. According to Empire Airlines’ GOM, “when light
freezing rain, light or moderate freezing drizzle, or light, moderate, or heavy snow is falling,
aircraft may land.” The GOM also stated that, “when light freezing rain, light to moderate
freezing drizzle, or light, moderate snow is falling, [an ATR] aircraft may take off, provided it is
prepared in accordance with approved deicing procedures.”
138
NTSB/SR-81/01.
139
NTSB/AAR-96/01.
140
For more information about the NPRM, see section 2.4.1.2.

NTSB Aircraft Accident Report
70
After the accident, on February 27, 2009, Empire Airlines issued a flight operations
bulletin to supersede the icing information in the GOM and to inform flight crews and flight
followers that freezing rain and freezing drizzle are not covered by the icing certification
envelope and that takeoff or landing operations in known or reported freezing rain or freezing
drizzle of any intensity are prohibited. An informal review of other 14 CFR Part 121 and 135
operators’ icing guidance revealed that the operators’ guidance for dispatching their
turbine-powered, pneumatic deice boot-equipped airplanes into freezing rain and freezing drizzle
conditions varied widely; some operators prohibited dispatch into such conditions, and others
permitted it.
As this accident shows, moderate icing conditions due to light freezing drizzle can
increase a flight crew’s workload and degrade the performance of the airplane. Although Empire
Airlines and the other FedEx feeder operators developed “no-go” weather guidance (after the
accident) that prohibits takeoff or landing operations in known or reported freezing rain or
freezing drizzle, these actions were not required by the FAA, and other operators may not adopt
such safety measures. The NTSB concludes that dispatching and operating an airplane in known
icing conditions for which the airplane is not certificated and has not demonstrated the ability to
operate safely has the potential to reduce or eliminate safety margins. Therefore, the NTSB
recommends that the FAA prohibit all 14 CFR Part 121, 135, and 91 subpart K operators of
pneumatic deice boot-equipped airplanes from dispatching or deliberately operating these
airplanes in known freezing rain or freezing drizzle of any intensity, unless the airplane
manufacturer has demonstrated that the airplane model can safely operate in those conditions.
2.4.1.1 Flight Crewmember and Dispatcher Training Related to Icing Conditions
According to Empire Airlines’ director of operations, the GOM information in place
before the accident (which permitted dispatching and operating airplanes in light freezing rain;
light or moderate freezing drizzle; or light, moderate, or heavy snow) was developed based on
information from the ADP holdover tables. However, the NTSB notes that holdover tables are
references that are used for ground deicing operations and are not intended to be used to address
the in-flight icing environment.
141
Interviews with Empire Airlines’ flight followers and the dispatch manager revealed that
their perceptions about dispatching into freezing drizzle conditions were based on this GOM and
ADP information. However, such guidance based on ground deicing operations did not
emphasize the potential dangers of in-flight encounters with freezing rain and freezing drizzle
that are described in airplane-specific flight operations publications. For example, the AFM for
the airplane (which is a flight publication provided by ATR) contained the following warning:
Severe icing may result from environmental conditions outside of those for which
the airplane is certificated. Flight in freezing rain, freezing drizzle, or mixed icing
141
In the section of the March 2011 edition of Cold Weather Operations: Be Prepared for Icing that discusses
ground deicing, ATR states, in part, the following: “IMPORTANT: The fluids used during ground de/anti-icing is
not intended for and does not provide protection during the flight. Before take-off, pilots must be aware of potential
in-flight severe icing conditions…. If such conditions exist, take-off must be delayed”

NTSB Aircraft Accident Report
71
conditions (supercooled liquid water and ice crystals) may result in ice buildup on
protected surfaces exceeding the capabilities of the ice protection system.
Also, ATR’s Cold Weather Operations publication
142
stated that in-flight icing is a major
concern for commuter airplanes (which are typically pneumatic deice boot-equipped airplanes)
in particular because they fly at altitudes where icing conditions are most likely to occur. Neither
of these flight publications was used in developing dispatch guidance.
Based on information obtained during interviews with flight crewmembers and dispatch
personnel, the NTSB found that many were not sufficiently aware of the dangers of operating in
freezing drizzle precipitation and lacked a thorough understanding of the weather phenomena
associated with SLD conditions. Although on March 16, 2010, the FAA issued SAFO 10006,
which referenced several of the NTSB’s safety recommendations that resulted from its
investigation of the October 31, 1994, accident in Roselawn, Indiana,
143
to encourage all
operators to review and amend, if necessary, their flight crewmember and dispatcher training
programs to ensure that their programs address SLD icing conditions, the actions recommended
in a SAFO are not mandatory. Also, as noted previously, other operators’ dispatch guidance
varied, and Empire Airlines erroneously relied on ground deicing guidance as the basis for
dispatch decisions, which resulted in assumptions that led to the dispatch of flights into freezing
drizzle without adequate consideration for the in-flight hazards associated with the conditions.
The NTSB is concerned that disparity exists between operators’ and airplane
manufacturers’ guidance materials and between the guidance materials of operators of similar
airplanes regarding flight operations in SLD conditions, particularly after the NTSB issued
numerous safety recommendations on the topic resulting from its investigation of the October 31,
1994, accident in Roselawn, Indiana.
144
Dispatch personnel like Empire Airlines’ flight
followers who authorize each flight release, provide preflight weather products, and perform
flight following share an integral role with flight crews in ensuring that each flight safely reaches
its destination. The NTSB concludes that, to most effectively ensure the safety of flight
operations in icing conditions, pilots, dispatchers, and flight followers must understand how the
dangers of freezing drizzle and freezing rain can affect their airplanes and must understand the
differences between ground deicing considerations and in-flight icing operations. Therefore, the
NTSB recommends that the FAA review the approved pilot, dispatcher, and flight follower
training programs and procedures for all 14 CFR Part 121, 135, and 91 subpart K operators and
require revisions to the programs and procedures, as necessary, to include standardized training
and aircraft-specific information to educate pilots, dispatchers, and flight followers of the
dangers of flight operations in freezing precipitation and of the differences between ground
deicing considerations and in-flight icing operations.
142
Cold Weather Operations: Be Prepared for Icing (2008).
143
NTSB/AAR-96/01.
144
NTSB/AAR-96/01.

NTSB Aircraft Accident Report
72
2.4.1.2 Proposed Rulemaking for Airplane Certification Requirements for Flight in
Icing Conditions
In response to several NTSB safety recommendations, on June 29, 2010, the FAA issued
an NPRM
145
intended to improve the safety of transport-category airplanes operating in SLD,
mixed-phase, and ice-crystal icing conditions. The NPRM included proposals for expanding the
certification icing environment for newly certificated transport-category airplanes to include
freezing rain and freezing drizzle and for requiring airplanes most affected by SLD icing
conditions to meet certain safety standards in the expanded certification icing environment,
including additional airplane performance and handling requirements.
On August 27, 2010, in comments submitted to the docket for this NPRM, the NTSB
stated that it was pleased that the NPRM proposed to add new sections to 14 CFR Part 25.
Specifically, the NTSB noted section 25.1420, which would require aircraft manufacturers to
evaluate airplane operation in the SLD environment, and Appendix O, Part I, which would
expand the certification icing environment to include freezing rain and freezing drizzle by using
four separate droplet-size distributions. Additionally, the NTSB stated that it was pleased to see
the inclusion of Appendix O, Part II, which states the following:
The most critical ice accretion in terms of airplane performance and handling
qualities for each flight phase must be used to show compliance with the
applicable airplane performance and handling qualities requirements for icing
conditions contained in Subpart B of this part. Applicants must demonstrate that
the full range of atmospheric icing conditions specified in Part I of this appendix
have been considered, including drop diameter distributions, liquid water content,
and temperature appropriate to the flight conditions.
Although the NTSB finds that several aspects of the FAA’s NPRM are essential for
improving the safety of flight for airplanes operating in icing conditions, the NTSB is
disappointed that the proposed rule applies only to newly certificated aircraft (thus, the accident
airplane would not be subject to the new rules) and that it excludes certain aircraft (such as those
with a maximum takeoff weight of more than 60,000 lbs or irreversible flight controls) from
compliance with the new safety standards. In its response, the NTSB noted that SLD conditions
can present a danger for the current fleet of aircraft; therefore, the proposed rule should be
expanded beyond newly certificated airplanes to include all deice boot-equipped airplanes
currently in service that are certificated for flight in icing conditions.
2.4.2 Training Program and Manual Discrepancies
Empire Airlines personnel indicated that, during basic indoctrination training, pilots
reviewed the ADP, FAA’s meteorology handbook, and icing videos. Empire Airlines personnel
also indicated that, during training at FlightSafety, pilots reviewed the ATR Cold Weather
Operations publication
146
and reviewed meteorological conditions likely to cause freezing
145
75 FR 37311-37339.
146
Cold Weather Operations: Be Prepared for Icing (2008).

NTSB Aircraft Accident Report
drizzle and freezing rain. However, Empire Airlines’ FTM included a document that indicated
that Empire Airlines (not FlightSafety) was required to provide the required meteorology
training, including the ATR publication, as part of the meteorology module. Interviews with
FlightSafety instructors revealed that they were not providing or using the publication during
training. The flight crew did not recall receiving this document.
Although Empire Airlines implemented special emphasis icing training for all ATR pilots
after the accident, the NTSB had concerns that the FAA did not detect these training program
discrepancies before the accident. Spokane FSDO personnel managed their oversight of Empire
Airlines through the FAA’s ATOS program. A review of the ATOS program table,
“System/Subsystem/Element Chart—Operations and Cabin Safety Elements,” revealed that, as
part of the program, the FAA was required to provide oversight of an airline’s FTM content and
flight crewmember training. However, the inspectors who followed the ATOS program did not
detect that Empire Airlines was not providing the required meteorology training, including the
ATR publication, as part of the meteorology training module. Upon learning of this, the FAA
contacted the certificate management offices of other ATR operators and determined that this
was an oversight problem in the inspection process at Empire Airlines and not a systemic issue
with ATOS. Additionally, the FAA took corrective action to assure that changes to Empire
Airlines’ FTM were initiated to assure that the required meteorological training was being
conducted by the operator.
2.5 Survival Aspects
According to dispatch logs, the accident alarm sounded at 0438:12. ARFF personnel who
were dispatched to the scene reported that they proceeded on the taxiways with caution because
of the ice. The ARFF response vehicles arrived on scene without difficulty at 0442:31, and
ARFF personnel immediately began fire suppression and contained the fire (with the exception
of a few interior cargo fires) within minutes. Thus, the NTSB concludes that the presence of ice
on the taxiways between the ARFF station and the accident site minimally increased the response
time; however, the emergency response was timely and effective in suppressing the fire.
2.5.1 Lack of Occupant and Hazardous Materials Information Available to First
Responders
The first officer opened the cockpit escape hatch without difficulty, but the flight crew
decided not to use it for egress because of the fire’s proximity. The captain and the first officer
opened the forward cargo door without difficulty and exited the airplane. The first officer stated
that, before exiting the airplane, the captain attempted to contact the ATCT using the airplane’s
radio but that the radio was inoperative (the CVR did not capture this attempt). The captain
stated that, after exiting the airplane, he called Empire Airlines’ dispatch and reported the
accident. Both the captain and the first officer then left the scene and ran to the FedEx hangar
before the first responders arrived. A FedEx employee subsequently notified the Lubbock Fire
Department and EMS personnel when they arrived at LBB that the flight crew was at the FedEx
hangar; however, by that time, the ARFF responders were already on scene and looking for
survivors.
73

NTSB Aircraft Accident Report
74
As a result of the confusion regarding the flight crewmembers’ whereabouts, at least two
ARFF personnel unnecessarily accessed the airplane to look inside the cockpit and cabin area,
and other personnel also unnecessarily interrupted their fire suppression activities to participate
in the search. After the arriving fire department personnel conveyed to ARFF personnel that the
flight crew was safe, the search was stopped but then was resumed briefly after the ATCT
controller relayed information (which was apparently old) that a pilot was walking around on the
ramp looking for assistance. In addition, the ARFF personnel were initially unaware of the
airplane’s HAZMAT cargo. Operators that transport HAZMAT cargo are required to make
specific HAZMAT cargo information available during an emergency response, and Empire
Airlines’ procedures complied with the requirements. However, the requirements do not address
situations in which the flight crew may be able to provide more timely, general information in
advance of the operator’s delivery of the required documents. The ARFF captain indicated that,
if they had the information, the ARFF response to the scene would have been similar with the
exception that all responding firefighters would have worn full personal protective equipment.
Although the flight crewmembers acted appropriately by ensuring their own safety
following the accident, the situation highlights that a lack of information from the flight crew can
hinder the response team’s ability to safely and most efficiently prioritize their on-scene
activities. The NTSB notes that a similar situation occurred on June 28, 2008, during a cargo
airplane ground fire in which the flight crew evacuated the airplane and left the scene before first
responders arrived, but no information about their safe egress was immediately provided to first
responders. In this accident, a firefighter unnecessarily entered the burning wreckage to look for
survivors and encountered a dangerous situation in the cockpit, including heavy smoke in which
he lost his radio, confined spaces that pulled off some of his equipment, and a “wall of fire”
behind the cockpit door. The firefighter indicated that, in hindsight, he should not have entered
the cockpit but that he did it because he did not know if anybody was in there and because he
thought that he could put the fire out.
147
The ARFF station was notified of the accident when the ATCT controller lifted the
direct-line radio receiver in the tower, resulting in the automatic sounding of a tone in the station.
According to procedure, following the tone, the ATCT controller can provide information about
the level of the alert, the type of aircraft, the nature of the emergency, the runway to be used, and
any other information as time permits. In the case of the accident flight, other than the accident
location, the only information about the flight that the ATCT controller could convey was that
the airplane was an ATR. ARFF personnel did not know that it was a cargo airplane and that
they could expect two or three occupants until they began suppressing the fire and saw the FedEx
logo on airplane’s tail. Further, as previously discussed, the ARFF responders were initially
unaware of the airplane’s HAZMAT cargo.
The NTSB concludes that timely information from the flight crew about the safety of the
airplane occupants and the presence of on-board HAZMAT cargo would improve the safety and
efficiency of the emergency response. Further, the NTSB concludes that, because flight crews
cannot always immediately communicate with ATC after an accident, it is important that another
147
See the Survival Factors Group Chairman’s Factual Report in the public docket for Ground Fire Aboard
Cargo Airplane, ABX Air Flight 1611, Boeing 767
‐
200, N799AX, San Francisco, California, June 28, 2008, Aircraft
Accident Summary Report NTSB/AAR-09/04/SUM (Washington, DC: National Transportation Safety Board,
2009). <http://www.ntsb.gov/Dockets/Aviation/DCA08MA076/407654.pdf>.

NTSB Aircraft Accident Report
method be developed to communicate information, such as the number of occupants on board
and the presence of hazardous materials, to ARFF personnel upon initial notification of an
accident. Therefore, the NTSB recommends that the FAA develop a method to quickly
communicate information regarding the number of persons on board and the presence of
hazardous materials to emergency responders when airport emergency response or search and
rescue is activated.
2.5.2 Inoperative Emergency Response and Mutual Aid Gate
The airport’s emergency plan indicated that units that respond from outside of the airport
should “respond to Gate 6 and Gate 48 or at a location prescribed by the command post.”
However, the emergency response unit that arrived at Gate 48 could not access the airport at that
location because the gate was inoperative due to ice in its operating mechanism. The remaining
response units were able to divert to another gate for airport access, which minimally delayed
their response time.
The LBB snow and ice removal plan did not address checking or ensuring the operability
of the airport gates. A survey of several other 14 CFR Part 139 airports with operations affected
by winter weather revealed that none of the airports’ snow and ice operations plans addressed
checking or ensuring the operability of emergency response and mutual aid gates. Also,
AC 150/5200-30C did not address the issue.
The NTSB notes that airport operations personnel are already required by airport snow
and ice removal plans to conduct periodic inspections of the routes used by emergency response
vehicles. Therefore, the checking of mutual aid gates for operability could easily be added as an
item to be performed during these inspections. Further, following the accident, LBB voluntarily
added the checking of mutual aid gates for operability to its snow and ice operations plan. The
NTSB concludes that an iced and inoperable mutual aid gate could extend the response time of
mutual aid, which could delay the delivery of medical attention to accident survivors and result
in further fire damage to property. Therefore, the NTSB recommends that the FAA amend
AC 150/5200-30C to include guidance on monitoring and ensuring the operability of emergency
response and mutual aid gates during winter operations.
2.6 Airplane Equipment Options
2.6.1 Aircraft Performance Monitoring
ATR developed the APM system, which has been installed on new production ATR 42
and ATR 72 airplanes since November 2005, to enhance a flight crew’s ability to detect the
effects of severe icing conditions on the airplane. The APM is a condition-specific, low-airspeed
alerting system because it is designed to provide specific alerts in icing conditions only (level 2
or 3 icing protection must be engaged or an icing signal must be provided by the icing detector).
The APM calculates and compares the airplane’s actual performance (with respect to airspeed
and drag) with its expected performance, computes the actual minimum icing and severe icing
airspeeds, and provides alerts to the flight crew when low airspeed or performance degradation is
detected. These alerts prompt the flight crew to perform the specified QRH procedures
75

NTSB Aircraft Accident Report
(depending upon the type of alert) to respond to the effects of icing on the airplane’s
performance.
Although the APM is intended to help flight crews recognize and respond to performance
degradations developed while operating in severe icing encounters, the APM alerts are an
important safety enhancement for flights operating even in moderate icing conditions, like the
accident flight. For example, had the accident airplane been equipped with an APM, the blue
“CRUISE SPEED LOW” annunciator lights would have illuminated about 70 seconds before the
flap anomaly, and the amber “DEGRADED PERF” annunciator lights and a single chime would
have activated about 40 seconds before the flap anomaly. An APM would not have provided any
further alerts after the flight crew selected flap extension because the system requires a flaps-up
configuration.
According to ATR, the appropriate flight crew response to the “DEGRADED PERF”
alert includes maintaining red-bug airspeed plus 10 kts. The NTSB notes that, although the
accident flight’s hazardous low-airspeed situation resulted from the flight crew’s inadequate
airspeed management rather than the performance degradation from the moderate icing
encounter, had the accident airplane been equipped with an APM, the APM would have provided
icing-related alerts that may have alerted the flight crew of the need to be more attentive to
airspeed management during the approach. Thus, the NTSB concludes that the APM system is a
valuable low-airspeed alerting tool that can enhance safety in all icing conditions.
APM retrofits for older ATR 42 (like the accident airplane) and ATR 72 airplanes have
been available since June 2006, and, effective August 24, 2009, EASA required that all
EASA-participating operators (operators in the European Community, its Member States, and
the European third countries) of ATR 42 and 72 airplanes not originally equipped with the APM
system retrofit their airplanes with the system within 72 months or by the second “C” check,
whichever occurs first. The FAA did not take similar action. As a result, APM system retrofits
are optional for U.S. operators.
In a January 14, 2011, letter responding to a query from NTSB investigators, the FAA
stated that its decision not to require APM retrofits for U.S. operators was based, in part, on its
finding that, in five of the ten icing-related events that were cited by EASA when mandating the
APM, the flight crewmembers were aware they were in severe icing conditions but did not
follow mandatory operating limitations. Therefore, the FAA reasoned that although the APM
would have provided alerts in four of these five cases, “it cannot be determined if the flight crew
would have acted any differently in response to an APM alert than they did to observing the
severe icing cues.” The NTSB notes that, in times of high workload, an alert even a few seconds
earlier that an ice accretion has crossed the line from “normal” to severe would be beneficial
because it would allow the flight crew to take immediate action. Because the APM warns of
performance degradations when they begin to occur, even if the autopilot is on and the crew is
unable to detect degradation in performance, the APM can provide warnings to flight crews that
a hazardous low-airspeed situation is developing well before the icing conditions become severe.
The NTSB does not concur with the FAA’s position that APMs would not help flight crews in
icing conditions and believes that the FAA should reexamine its decision not to require APM
retrofits for U.S. operators. Therefore, the NTSB recommends that the FAA require all operators
76

NTSB Aircraft Accident Report
of ATR 42- and ATR 72-series airplanes to retrofit the airplanes with an APM system if they are
not already so equipped.
2.6.2 Flap Malfunction or Asymmetry Light
During the accident flight, the flap asymmetry was not quickly or accurately identified by
either flight crewmember, despite several available cues, including the cockpit flap position
indicator, the exterior wing flap position fairings, the left control wheel input by the autopilot
(and the resulting 5° heading change of the airplane), the airplane’s failure to decelerate as
expected, and the “RETRIM ROLL L WING DN” and “AILERON MISTRIM” messages on the
ADU. Although it is possible that the flight crewmembers did not detect all of the cues (both the
captain and the first officer stated that they did not see any messages on the ADU), the cues they
did observe were not rapidly interpreted as indicative of a flap problem.
The NTSB notes that the ATR 42-320 (the accident airplane model) is one of only a few
models of transport-category airplanes certificated without a flap malfunction light (either a light
to indicate any flap malfunction or a specific asymmetry light) in the cockpit (other models are
the ATR 42-200 and -300 and the Cessna 500, 550, 553, 560, and 560XL airplanes).
Certification testing for these airplanes demonstrated that a cockpit light was not required
because a flap malfunction (including an asymmetry) did not constitute an unsafe flight
condition.
If the accident airplane had been equipped with a flap malfunction light in the cockpit,
the light would have illuminated amber in response to the flap asymmetry and would have
provided the flight crew with an immediate, definitive indication of a flap problem. The NTSB
concludes that, if the accident airplane had been equipped with a flap asymmetry light, as many
other ATR 42- and ATR 72-series airplanes are equipped, the illumination of that light would
likely have made the nature of the malfunction more salient to the flight crew and may have
triggered a more appropriate crew response. Therefore, the NTSB recommends that the FAA
require that all ATR 42-series airplanes be equipped with a flap asymmetry annunciator light if
they are not already so equipped.
2.6.3 Ice Evidence Probe
The accident airplane was not equipped with an IEP, which was an optional installation
for ATR airplanes that were not originally equipped with this device. Although an IEP provides a
surface upon which ice accumulation can be visually detected, the propeller spinners serve this
function for airplanes that are not equipped with an IEP, and the first officer indicated that she
observed ice on the spinners. Also, the AAS alerted the flight crew in a timely manner to apply
the procedures and checklists required when flying in icing conditions. Thus, the NTSB
concludes that the absence of an IEP, which was an optional installation, did not hinder the flight
crew’s ability to detect airframe ice accretion.
77

NTSB Aircraft Accident Report
78
2.7 Simulator Training for Icing Encounters
During the accident flight, both the flap asymmetry and the airframe ice accretion
adversely affected the airplane’s performance. Aerodynamic coefficient extraction indicated that
drag beyond the level expected for an uncontaminated airframe was present during cruise and the
final minutes of the flight. ATR estimated that, by the time that the flap asymmetry occurred, a
drag increase (due to ice) corresponding with about 23 percent of total power was present. The
EFS could not reproduce the accident airplane’s drag levels from ice accretion without
introducing unrealistic lift and pitch, roll, and yaw moments; therefore, the full extent of the
performance degradations could not be determined or duplicated in the EFS. No requirements
exist for simulators to be qualified with validated data, such as flight test and FDR data, for the
effects of airframe ice accumulation.
In this accident, the airplane’s stall warning system operated as designed and warned the
flight crew of the airplane’s proximity to the stall. However, other accidents and incidents have
occurred in which airframe ice accumulation has resulted in airplanes entering an aerodynamic
stall without any warning to the flight crews. For example, on January 2, 2006, a Saab SF340
operated by American Eagle Airlines, Inc., encountered icing conditions during the en-route
climb and departed controlled flight at an altitude of about 11,500 feet msl, losing about
5,000 feet of altitude before the pilots recovered control of the airplane.
148
The flight crew was
using the autopilot in vertical speed mode at the time that airplane control was lost, and
information from the FDR showed that the upset began before the stall warning activated.
The performance degradations associated with airframe ice accretion can result in an
aircraft slowing down much faster than normal and stalling at a much higher airspeed than
normal. Both conditions require pilot vigilance to recognize and react to the performance
degradations; however, both the American Eagle incident flight crew and this accident flight
crew failed to properly monitor and manage the airplanes’ airspeed. Although flight crews are
trained to use higher airspeeds during icing conditions, the effects of performance degradations
resulting from ice accretion are not realistically duplicated in a simulator.
The NTSB concludes that simulator-based training scenarios that realistically reflect
aircraft performance degradations that result from airframe ice accretion can better prepare flight
crews to effectively respond to decaying airspeed situations and other situations that can occur
during in-flight icing encounters. Therefore, the NTSB recommends that the FAA define and
codify minimum simulator model fidelity requirements for aerodynamic degradations resulting
from airframe ice accumulation. These requirements should be consistent with performance
degradations that the NTSB and other agencies have extracted during the investigations of icing
accidents and incidents.
The NTSB further recommends that the FAA, once the simulator model fidelity
requirements requested in Safety Recommendation A-11-46 are implemented, require that flight
crews of all aircraft certificated for flight in icing conditions be trained in flight training
simulators that meet these fidelity requirements. Such simulation training should emphasize the
148
The report for this incident, NTSB case number LAX06IA076, is available online at
<http://www.ntsb.gov/aviationquery/index.aspx>.

NTSB Aircraft Accident Report
following: (1) cues for recognizing changes in the aircraft’s flight characteristics as airframe
icing develops; (2) procedures for monitoring and maintaining appropriate airspeeds in icing
conditions, including the use of icing airspeed reference indices; and (3) procedures for
responding to decaying airspeed situations, stall protection system activation, and early stalls that
can occur without stall protection system activation.
79

NTSB Aircraft Accident Report
3. Conclusions
3.1 Findings
1. The captain and the first officer were certificated in accordance with Federal regulations and
were current and qualified in accordance with Empire Airlines’ training requirements. The
investigation found no evidence that the pilots’ performance was affected by any behavioral
or medical condition, or by the use of alcohol or drugs.
2. The airplane was loaded within weight and center of gravity limits and was maintained in
accordance with 14 Code of Federal Regulations Part 121.
3. The investigation found no evidence that indicated any mechanical anomaly with the
engines, and flight data recorder data indicated that the engines’ performance was consistent
with normal operations.
4. Performance data indicated that, when the flight crew commanded 15° flaps, a flap
asymmetry occurred with the left flaps extending 8° to 10° and the right flaps not extending.
The data further indicated that the flaps returned to a symmetric state (about 4.5°) about
25 seconds before ground impact.
5. Because of the extent of the impact and postaccident fire damage to the right flaps and flap
actuators, the reason for the airplane’s flap asymmetry could not be determined.
6. The airplane was controllable with the flap asymmetry and airframe ice contamination and
could have been maneuvered and landed safely if the appropriate airspeed had been
maintained.
7. The captain’s failure to immediately respond to the aural stall warning, the stick shaker, and
the terrain awareness and warning system warning resulted in his inability to arrest the
airplane’s descent and avoid impact with the ground.
8. The captain was adequately trained on how to respond to flap anomalies, and the captain’s
statement that the airplane had “no flaps” indicates that he had sufficient information to
recognize that he should immediately perform a go-around maneuver and apply the
appropriate procedure from the quick reference handbook that applied to all flap problems.
9. Although the captain indicated that he was concerned about the icing conditions, the presence
of airframe ice accretion within the capabilities of the airplane’s systems does not negate the
importance of adhering to standard operating procedures and performing a go-around
maneuver to respond to the multiple cues associated with an unstabilized approach including
excessive deviation from the glidepath, sink rate greater than 1,000 feet per minute, and
airspeed less than the required approach speed.
80

NTSB Aircraft Accident Report
10. Had the captain complied with standard operating procedures in response to the flap
anomaly, unstabilized approach, stick shaker, and terrain awareness and warning system
warning and initiated a go-around maneuver, the accident likely would not have occurred.
11. The first officer’s failure to maintain airspeed while acting as the pilot flying likely resulted
from being distracted by the flap anomaly, the captain’s actions in response to it, and the
control force inputs needed to maintain aircraft control.
12. The captain’s failure to call out the first officer’s airspeed deviations resulted directly from
his preoccupation with performing an inappropriate, nonstandard procedure in response to
the flap anomaly.
13. Although some of the airspeed bugs (including the internal bug) were not set to the
appropriate approach airspeeds and were not reset following recognition of the flap anomaly,
the flight crew had a sufficient reference to maintain the minimum safe airspeed because the
airspeed for a no-flap approach in icing conditions was correctly briefed as 143 knots, and
the red airspeed bugs were set near that value.
14. Reliance upon flight crew vigilance and stall warning systems may be inadequate to prevent
hazardous low-airspeed situations, and, had a low-airspeed alerting system been installed on
the airplane, it may have directed the flight crew’s attention to the decaying airspeed earlier
and provided an opportunity to take corrective action before the stall protection system
activated.
15. The first officer’s failure to assert herself to the captain and initiate a go-around maneuver
when she recognized the unstabilized approach likely resulted from the steep authority
gradient in the cockpit and the first officer’s minimal training on assertiveness; further, the
captain’s quick dismissal of the first officer’s go-around inquiry likely discouraged the first
officer from voicing her continued concerns and challenging the captain’s decision to
continue the unstabilized approach.
16. Role-playing exercises are essential for effective assertiveness training because such
exercises provide flight crews with opportunities for targeted practice of specific behaviors
and feedback that a lecture-based presentation format lacks.
17. The establishment of best practices for conducting both single and multiple emergency and
abnormal situations training needs to include training for the occurrence of these situations at
low altitudes because low-altitude scenarios require rapid, accurate assessment of abnormal
situations and appropriate prioritization of tasks.
18. Although the risk for fatigue existed at the time of the accident due to the window of
circadian low, the first officer took steps to mitigate the effects of fatigue, and her errors
during the flight can be explained by her lack of experience in both the airplane and in icing
conditions along with the distraction caused by the captain’s non-standard response to the
flap anomaly.
19. Due to the early morning hour of the accident flight and cumulative sleep debt, it is likely
that fatigue degraded the captain’s performance.
81

NTSB Aircraft Accident Report
20. Dispatching and operating an airplane in known icing conditions for which the airplane is not
certificated and has not demonstrated the ability to operate safely has the potential to reduce
or eliminate safety margins.
21. To most effectively ensure the safety of flight operations in icing conditions, pilots,
dispatchers, and flight followers must understand how the dangers of freezing drizzle and
freezing rain can affect their airplanes and must understand the differences between ground
deicing considerations and in-flight icing operations.
22. The presence of ice on the taxiways between the aircraft rescue and firefighting station and
the accident site minimally increased the response time; however, the emergency response
was timely and effective in suppressing the fire.
23. Timely information from the flight crew about the safety of the airplane occupants and the
presence of on-board hazardous materials cargo would improve the safety and efficiency of
the emergency response.
24. Because flight crews cannot always immediately communicate with air traffic control after
an accident, it is important that another method be developed to communicate information,
such as the number of occupants on board and the presence of hazardous materials, to aircraft
rescue and firefighting personnel upon initial notification of an accident.
25. An iced and inoperable mutual aid gate could extend the response time of mutual aid, which
could delay the delivery of medical attention to accident survivors and result in further fire
damage to property.
26. The aircraft performance monitoring system is a valuable low-airspeed alerting tool that can
enhance safety in all icing conditions.
27. If the accident aircraft had been equipped with a flap asymmetry light, as many other
ATR 42- and ATR 72-series airplanes are equipped, the illumination of that light would likely
have made the nature of the malfunction more salient to the flight crew and may have
triggered a more appropriate crew response.
28. The absence of an ice evidence probe, which was an optional installation, did not hinder the
flight crew’s ability to detect airframe ice accretion.
29. Simulator-based training scenarios that realistically reflect aircraft performance degradations
that result from airframe ice accretion can better prepare flight crews to effectively respond
to decaying airspeed situations and other situations that can occur during in-flight icing
encounters.
82

NTSB Aircraft Accident Report
3.2 Probable Cause
The National Transportation Safety Board determines that the probable cause of this
accident was the flight crew’s failure to monitor and maintain a minimum safe airspeed while
executing an instrument approach in icing conditions, which resulted in an aerodynamic stall at
low altitude. Contributing to the accident were 1) the flight crew’s failure to follow published
standard operating procedures in response to a flap anomaly, 2) the captain’s decision to
continue with the unstabilized approach, 3) the flight crew’s poor crew resource management,
and 4) fatigue due to the time of day in which the accident occurred and a cumulative sleep debt,
which likely impaired the captain’s performance.
83

NTSB Aircraft Accident Report
4. Recommendations
As a result of this investigation, the National Transportation Safety Board makes the
following recommendations to the Federal Aviation Administration:
Require that role-playing or simulator-based exercises that teach first officers to
assertively voice their concerns and that teach captains to develop a leadership
style that supports first officer assertiveness be included as part of the already
required crew resource management training for 14 Code of Federal Regulations
Part 121, 135, and 91 subpart K pilots. (A-11-39)
Prohibit all 14 Code of Federal Regulations Part 121, 135, and 91 subpart K
operators of pneumatic deice boot-equipped airplanes from dispatching or
deliberately operating these airplanes in known freezing rain or freezing drizzle of
any intensity, unless the airplane manufacturer has demonstrated that the airplane
model can safely operate in those conditions. (A-11-40)
Review the approved pilot, dispatcher, and flight follower training programs and
procedures for all 14 Code of Federal Regulations Part 121, 135, and 91
subpart K operators and require revisions to the programs and procedures, as
necessary, to include standardized training and aircraft-specific information to
educate pilots, dispatchers, and flight followers of the dangers of flight operations
in freezing precipitation and of the differences between ground deicing
considerations and in-flight icing operations. (A-11-41)
Develop a method to quickly communicate information regarding the number of
persons on board and the presence of hazardous materials to emergency
responders when airport emergency response or search and rescue is activated.
(A-11-42)
Amend Advisory Circular 150/5200-30C to include guidance on monitoring and
ensuring the operability of emergency response and mutual aid gates during
winter operations. (A-11-43)
Require all operators of Avions de Transport Régional Aerospatiale Alenia
ATR 42- and ATR 72-series airplanes to retrofit the airplanes with an aircraft
performance monitoring system if they are not already so equipped. (A-11-44)
Require all Avions de Transport Régional Aerospatiale Alenia ATR 42-series
airplanes to be equipped with a flap asymmetry annunciator light if they are not
already so equipped. (A-11-45)
Define and codify minimum simulator model fidelity requirements for
aerodynamic degradations resulting from airframe ice accumulation. These
requirements should be consistent with performance degradations that the
84

NTSB Aircraft Accident Report
National Transportation Safety Board and other agencies have extracted during
the investigations of icing accidents and incidents. (A-11-46)
Once the simulator model fidelity requirements requested in Safety
Recommendation A-11-46 are implemented, require that flight crews of all
aircraft certificated for flight in icing conditions be trained in flight training
simulators that meet these fidelity requirements. Such simulation training should
emphasize the following: (1) cues for recognizing changes in the aircraft’s flight
characteristics as airframe icing develops; (2) procedures for monitoring and
maintaining appropriate airspeeds in icing conditions, including the use of icing
airspeed reference indices; and (3) procedures for responding to decaying airspeed
situations, stall protection system activation, and early stalls that can occur
without stall protection system activation. (A-11-47)
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
DEBORAH A.P. HERSMAN ROBERT L. SUMWALT
Chairman Member
CHRISTOPHER A. HART MARK R. ROSEKIND
Vice Chairman Member
EARL F. WEENER
Member
Adopted: April 26, 2011
Vice Chairman Hart and Members Rosekind and Weener filed the following statements
on May 9, 2011.
85
NTSB Aircraft Accident Report
86
Board Member Statements
Vice Chairman Christopher A. Hart, dissenting:
I dissent from this report because (a) it is internally inconsistent, and (b) it concludes,
without adequate basis, that fatigue contributed to the accident.
Internal Inconsistency. The report is internally inconsistent because, on one hand, it
emphasizes the general rule, and the probable cause asserts, that the captain should have
discontinued his approach when it became unstable. On the other hand, it recommends that the
FAA should prohibit these types of airplanes “from dispatching or deliberately operating” in
precisely the type of icing conditions that it says this captain should have re-entered in his
go-around. Either the conditions were flyable and should have been re-entered on a go-around, or
the conditions were not flyable and the captain appropriately continued his approach, despite
being unstable, but not both.
1
I believe that the evidence supports the conclusion that the
conditions were flyable and the captain should have gone around.
More specifically, the evidence indicates that the icing conditions encountered during the
approach were well within the capability of the airplane and the crew. The crew had
appropriately engaged the necessary ice protection systems, they never expressed any concern
about icing, and the airplane had plenty of performance despite the icing. Thus, instead of being
an icing accident, this was an accident involving an unstable approach that resulted from
untimely and excessive corrections, along with poor CRM, during an instrument approach, and
there is no basis in the report for concluding that icing was in any way causal or even
contributory to this accident.
With a few small exceptions, the flight crew appeared to be working well together and
was generally “ahead of the curve” until they began to descend when the autopilot intercepted
the glide slope. Because the copilot (who was the pilot flying) did not reduce the power as their
descent began, the airplane began to accelerate. Her response to the acceleration was to reduce
power very substantially, essentially to flight idle. Making large corrections during an instrument
approach is not good practice because large corrections usually necessitate subsequent large
corrections in the opposite direction, which, as occurred here, can easily lead to an unstable
approach. About fifteen seconds after the autopilot intercepted the glide slope and they began
descending, and about ten seconds after she substantially reduced the power, something
happened – the investigation apparently was not able to determine with certainty what – that
caused the copilot to ask, at 0435:03, “what the heck is going on?” Her question may have been
prompted by the airplane’s reaction(s) to their effort to extend the flaps because, one second
later, the captain responded, “You know what? We have no flaps.”
Consequently, as they were rapidly decelerating during their descent along the glide
slope, her inquiry and the captain’s response about the flaps caused both pilots to divert their
1
The recommended prohibition against “dispatching” into icing conditions is proactive and appropriate, and
does not create an inconsistency. The recommended prohibition against “deliberately operating” in icing conditions,
however, flies in the face of asserting that the captain should have aborted his approach and re-entered the prohibited
icing conditions.
NTSB Aircraft Accident Report
attention to the flap problem. The captain, as pilot monitoring, appropriately began to trouble
shoot, but inappropriately began looking at circuit breakers rather than the flap malfunction
checklist. The copilot, however, was also distracted by the flap problem, which diverted her
attention away from their decreasing airspeed until it decreased enough to activate the stick
shaker and disconnect the autopilot. The copilot’s diversion of her attention was contrary to good
CRM practice that in the event of a malfunction, one pilot should explore the malfunction,
preferably starting with the checklist where appropriate, while the other pilot flies the airplane.
After the autopilot disconnected, the approach became unstable, they did not maintain adequate
airspeed, even after the stick shaker activated, and the airplane stalled and crashed.
Hence, this accident actually began with the copilot’s failure to reduce power when they
intercepted the glide slope, followed by her excessive power reduction in response to the
resulting acceleration, followed by the distraction caused by the flap problem that diverted her
attention – until the first stick shaker event – from the need to restore adequate power to prevent
further loss of speed. Because none of the events in this causal chain related to or were caused by
icing, this is not an icing accident, and there is no basis from this accident for any
recommendations regarding icing.
The higher stall speed due to icing does not undercut my conclusion that this is not an
icing accident. The copilot’s substantial power reduction caused an initial deceleration of about
2 knots per second, and I am not convinced, for two reasons, that the few additional seconds it
would have taken for them to decelerate to a lower (non-iced) stall speed might have produced a
different result. First, I see no reason to believe that those extra few seconds would have been
enough to cause them to return their attention – before the stall – to the need to arrest their rapid
speed decrease. Second, given their lack of appropriate response – not one, not two, but three
times – to the stick shaker, I see no basis for concluding that that those extra seconds would have
altered their non-response to the stick shaker.
Consequently, I do not believe that this was an icing accident, and
‐ The fact that they were in icing conditions is not relevant to, and should not be in, the
probable cause;
‐ The recommendations relating to in-flight icing, irrespective of whether they are
good ideas, are not supported by this accident; and
‐ Because Recommendation No. 2 asks the FAA to prohibit operation in the types of
icing conditions that were present in this accident, the probable cause should not
assert that the captain should have discontinued his approach and ascended back into
those icing conditions.
Fatigue. The probable cause concludes that fatigue “likely impaired the captain’s
performance.” Even if the crew had been fatigued, which they probably were to some extent, I
do not see any basis in the report for concluding that fatigue resulted in impairment sufficient to
cause or contribute to this accident.
There are several aspects about fatigue that necessitate extreme caution before including
it as part of the probable cause. To name a few, fatigue:
87

NTSB Aircraft Accident Report
‐ Is not either “on” or “off,” but can range from none, to extreme, to anywhere in
between;
‐ Can be quite variant from day to day, and can be present one day, enough to cause
problems, but not be present to that extent the next day; and it can even be quite
variant in the course of a single flight, depending upon the duration of the flight and
events during the flight;
‐ Is very widespread – at any point in time, a large percentage of the population is
probably suffering from fatigue to some extent;
‐ Is multidimensional – it is usually referred to in relation to sleep deficit, but it is also
affected by diet, exercise, smoking, alcohol use, age, and other factors, and the
impacts and interrelationships among and between those factors are often not well
understood;
‐ Is not directly measurable – it can be ascertained only indirectly, on the basis of
actions and behavior;
‐ Has effects that can arguably be counteracted by processes that are designed to reduce
the need to analyze and think, such as standard operating procedures and checklists;
‐ May be significantly mitigated, at least temporarily to some extent, by an adrenalin
rush in a life-threatening situation; and
‐ May be overwhelmed by the effects of a life-threatening situation.
Given all of these characteristics and uncertainties, caution is warranted regarding the
inclusion of fatigue as part of probable cause because, among other reasons, the incomplete
understanding of, and inability to measure, fatigue and its effects make it very difficult to
conclude that fatigue is causative; and given how widespread fatigue is, query how much our
inclusion of it in the probable cause can help us achieve our ultimate objective, which is the
issuance of safety-improving recommendations.
In this accident, there is probably ample basis for concluding, based upon sleep alone,
that both crewmembers were fatigued to some extent. Less ascertainable, however, is whether
their performance was degraded by fatigue enough to be causal or contributory to the accident.
As noted above, the flight crew appeared to be working well together and was generally “ahead
of the curve,” with a few small exceptions, until the autopilot intercepted the glide slope and they
neglected to reduce power when they began their descent. Their satisfactory behavior during
most of the flight could support the conclusion that their fatigue was not enough to impair their
performance, at least in the earlier stages of the flight. Another possible conclusion, however, is
that even if their fatigue were sufficient to impair their performance, their use of standard
operating procedures and checklists earlier in the flight may have masked the impairment effects.
Yet a third possible conclusion is that, even if fatigue did not measurably impair their
performance earlier in the flight, it degraded their performance later in the flight enough to be
causal or contributory. These varying and not necessarily consistent conclusions that can be
drawn from the evidence demonstrate the difficulty of labeling fatigue as causal to performance
impairment.
88
NTSB Aircraft Accident Report
Another complication derives from the fact that this was a life-threatening experience for
the crew. We can probably conclude with some confidence that the crew in this accident
considered their situation to be life-threatening, perhaps starting with her query, “What the heck
is going on?” at 0435:03, followed by his response, at 0435:04, “You know what? We have no
flaps.” Her question and his answer occurred only 84 seconds before the airplane impacted the
ground, during about half of which time they were out of the clouds and were able to see the
lighted runway and ground rapidly approaching.
At least two possibilities come to mind from the fact that the experience was life-
threatening. First, the crew probably experienced an adrenaline rush, and the adrenaline may
have reduced the impairing effects of fatigue, at least temporarily, in the critical final seconds
before impact. I am not aware of any literature on this issue, but intuitively it seems very
possible that adrenaline could, at least temporarily, counteract some of the potentially impairing
effects of fatigue. Second, their behavior in the final seconds before impact may have been so
overwhelmingly influenced by their knowledge that they were in a life-threatening situation that
the effects of fatigue were insignificant by comparison.
Given this extent of uncertainty, I do not believe that we have adequate basis for
concluding in the probable cause that fatigue “likely impaired the captain’s performance.”
89

NTSB Aircraft Accident Report
Member Mark R. Rosekind, concurring:
This accident has generated a constructive debate among the staff and Board Members on
several key issues, one of which is fatigue. Such debates support a thorough analysis and are at
the core of the NTSB’s mission. I commend the staff and fellow Board Members for raising
these issues.
This accident involved night shift work, circadian lows, and misconceptions regarding
the ability to adjust to overnight operations. As the report adequately sets forth, this accident
occurred during the window of circadian low at about 0437. Well-established scientific research
demonstrates that this time is associated with severe performance reductions, and increased
errors, incidents, and accidents. As a result, accidents involving pilot error that occur within this
window of time should be thoroughly examined for fatigue. While mitigation strategies can be
employed to somewhat counter the performance impairments caused by fatigue, overnight
operations will always be inherently more at risk due to the human body’s internal circadian
clock.
Scientific research has shown that the circadian clock does not fully adjust to night
operations over time without very specific interventions that require ideal conditions and are
very difficult to achieve. These targeted interventions require specific manipulation of light/dark
exposure and sleep which runs counter to our society.
In this accident, both pilots altered their sleep schedules in an effort to adjust their
circadian rhythms to their night flying operations. There was no information that either pilot had
received education and training about these interventions or had knowledge of the specific
actions required to shift circadian rhythms. The First Officer made a more extensive effort to
adjust her schedule and maintained it for a longer period of time. Despite these actions, no
information indicated she sufficiently employed mitigation strategies to effectively adjust her
circadian clock. For example, there is insufficient information to assess her light exposure or
whether she slept continuously during her sleep opportunity periods.
While I voted for and supported the conclusions set forth in the report, this concurring
statement is written, in part, to disagree with the conclusion that the First Officer’s errors “can be
explained by her lack of experience in both the airplane and in icing conditions along with the
distraction caused by the captain’s nonstandard response to the flap anomaly” (Conclusion 18).
The evidence that fatigue contributed to her errors is no less than the evidence suggesting that
her lack of experience or the Captain’s nonstandard response contributed to the accident.
Finally, this accident exemplifies the increased safety-risks associated with overnight
shifts and operations during the window of circadian low (at a minimum between 0300 and
0500) and should guide hours of service regulations, scheduling policies and practices, and
safety –sensitive operations affected by circadian factors.
90

NTSB Aircraft Accident Report
Member Earl F. Weener, concurring in part and dissenting in part:
Generally, I agree with the report and recommendations of Notation 8093B, as presented
to the Board on Tuesday, April 26, 2011. However, I cannot support the Probable Cause
statement, as adopted by the Board, or conclusion number 19.
As discussed at the Board meeting, I am unconvinced the investigation or final report
provides sufficient evidence to conclude that fatigue impaired the captain’s performance to the
extent it can be considered a cause of this accident, not even as a contributory factor.
I agree the captain may very well have experienced fatigue, and fatigue may have even
played a role in his performance. However, based on the evidence provided in this case, and as
presented in the final report, the causal connection between fatigue and the actions leading to this
accident has not been made.
Probable, as the word implies, means more than simply a possibility. The report initially
states that sleep needs vary by individual (p. 66). It then identifies several possibilities to explain
the captain’s performance, including past behavior and stress, along with fatigue. From this
observation the report concludes that the captain was “likely experiencing some fatigue at the
time of the accident,” (emphasis added) (p. 67), and that “fatigue likely degraded his
performance” (emphasis added) (p. 68). However, the report fails to provide an explanation for
why the possibility of fatigue is any more likely or probable than the other possibilities initially
identified. There is an unaccounted leap from several possibilities to explain the captain’s
performance to the singular conclusion that fatigue likely degraded the captain’s performance to
the extent it became a contributing causal factor of the accident. Further, the report fails to
explain how “likely experiencing some fatigue” becomes “likely degraded his performance.”
These conclusions, possibilities at best, do not support a finding of probability.
The immediate sequence of events leading to the accident began when the First Officer
(FO) mismanaged thrust at the interception of the glide slope. This was followed by loss of
airspeed leading to activation of stick-shaker and the subsequent disconnect of the autopilot. The
FO then had difficulty tracking the ILS localizer and glideslope and quickly deviated from the
ILS approach path to the point where the Captain asked if he should take over the approach. At
that point, the captain took manual control of an airplane that was likely out of trim and at a
power setting inconsistent with the intended ILS flight path. The airmanship errors committed by
the FO were certainly on the order of those subsequently made by the captain. Yet, staff
conclude that only the captain’s errors were likely caused by fatigue, while the FO’s were not.
In my opinion, nothing in the report substantiates this difference.
The report does discuss, in great detail, the FO’s actions, which, in turn, substantiates the
conclusion that her errors can be explained by lack of experience. However, the same level of
detail and analysis is lacking in terms of evaluating the captain’s actions. In fact, it is quite a
stark comparison. Also, the report cites a number of authoritative studies concerning the effects
of fatigue on human performance. However, the correlation of the studies to the crew’s
performance, is ambiguous. The report even acknowledges that the flight crew’s failure to
monitor air speed, the identified probable cause of this accident, could be consistent with the
known effects of fatigue; and at the same time, the report notes, the same error has been made by
91

NTSB Aircraft Accident Report
other crew who were not fatigued (p. 68). Again, at best, fatigue is one of several possibilities
that could explain the captain’s performance.
Further, when questioned on these points during the Board Meeting, staff again stated
that fatigue was one of a number of possibilities that could explain the captain’s performance,
and that indeed, it could also be explained by past behavior. The critical basis staff provided for
concluding that fatigue was a likely cause of the behavior, was an analysis derived by using the
captain’s own judgment that he required 6-8 hours of sleep to “feel rested,” and choosing to use
the more conservative end of this range, 8 hours, to arrive at a calculation of a sleep debt of 4
hours. However, I point out that in the initial draft of this report, fatigue was not identified as a
causal issue in this investigation. In fact, in briefings with staff in preparation for the Board
meeting, staff made a point of stating that they did analyze the role of fatigue in this accident and
ruled it out as a factor, as demonstrated in the initial report. When questioned at the Board
meeting on why this determination changed, staff explained that in the initial analysis they chose
to use the lower end of the captain’s sleep need range, 6 hours, to conduct the analysis and
subsequently determined fatigue did not play a role. Candidly, when the outcome of whether a
factor contributed to the cause of an accident is dependent on choosing from within a range, the
analysis is inconclusive.
Finally, I note the probable cause statement in the final draft of the report states the
probable cause for this accident was the flight crew’s failure to monitor and maintain a minimum
safe airspeed while executing an instrument approach in icing conditions. I further note the
original contributing factors to the accident in the initial draft report were limited to: 1) the flight
crew’s failure to follow published standard operating procedures in response to a flap anomaly;
2) the captain’s decision to continue with the unstabilized approach; and 3) the flight crew’s poor
crew resource management. All of these factors are supported by observable actions or inactions.
They were objectively derived, and not one of them is described as simply “likely” to have
occurred.
In sum, the report and probable cause, as initially proposed, provided a rational and
substantiated explanation for the cause of the accident. Although fatigue may have played a role
in the captain’s performance during the accident sequence, the final report does not sufficiently
make the case that fatigue played a causal role in the event.
92
NTSB Aircraft Accident Report
5. Appendixes
Appendix A
Investigation and Hearing
Investigation
The National Transportation Safety Board (NTSB) was notified about the accident on
January 27, 2009. Staff from the NTSB arrived on scene that same day and remained there until
January 30, 2009, to conduct the field portion of the investigation. No Board Member
accompanied the team.
In accordance with the provisions of Annex 13 to the Convention on International Civil
Aviation, the NTSB’s counterpart agencies in France and Canada, the Bureau d’Enquêtes et
d’Analyses (BEA) and the Transportation Safety Board (TSB), participated in the investigation
as the representatives of the State of Design and Manufacture (Airframe and Powerplants,
respectively). Avions de Transport Régional (ATR) and the European Aviation Safety Agency
(EASA) participated as technical advisors to the BEA. Pratt & Whitney, Canada, participated as
a technical advisor to the TSB.
Parties to the investigation were the Federal Aviation Administration (FAA); Empire
Airlines, Inc.; and FedEx Corporation.
Public Hearing
A public hearing was held on September 22 and 23, 2009, in Washington, D.C. Chairman
Deborah A.P. Hersman presided over the hearing.
The issues presented at the public hearing included flight crew procedures, crew resource
management and decision making, the airline’s training program for flight in icing conditions,
and airplane design modifications to monitor and mitigate the effects of icing on airplane
performance. Parties to the public hearing were the FAA, Empire Airlines, and ATR.
93
NTSB Aircraft Accident Report
Appendix B
Cockpit Voice Recorder Transcript
The following is a transcript of transcript of a Fairchild Model A-100A tape CVR, serial
number 59653, installed on an Empire Airlines ATR-42-320 (N902FX), which crashed during
landing at Preston Smith International Airport in Lubbock, Texas.
LEGEND
CAM Cockpit area microphone voice or sound source
HOT Flight crew audio panel voice or sound source
RDO Radio transmissions from N902FX
CTR Radio transmission from Dallas center controller
APR Radio transmission from the Lubbock approach controller
TWR Radio transmission from the Lubbock tower controller
OPS Radio transmission from Lubbock FedEx Operations
TAWS Terrain Awareness and Warning System sound source
-1 Voice identified as the captain
-2 Voice identified as the first officer
-? Voice unidentified
* Unintelligible word
# Expletive
@ Non-pertinent word
( ) Questionable insertion
[ ] Editorial insertion
Note 1: Times are expressed in CST.
Note 2: Generally, only radio transmissions to and from the accident aircraft were transcribed.
Note 3: Words shown with excess vowels, letters, or drawn out syllables are a phonetic representation of the words
as spoken.
Note 4: A non-pertinent word, where noted, refers to a word not directly related to the operation, control or condition
of the aircraft.
94

NTSB Aircraft Accident Report
95
CVR Quality Rating Scale
The levels of recording quality are characterized by the following traits of the cockpit voice recorder
information:
Excellent Quality Virtually all of the crew conversations could be accurately and easily understood.
The transcript that was developed may indicate only one or two words that were
not intelligible. Any loss in the transcript is usually attributed to simultaneous
cockpit/radio transmissions that obscure each other.
Good Quality Most of the crew conversations could be accurately and easily understood. The
transcript that was developed may indicate several words or phrases that were
not intelligible. Any loss in the transcript can be attributed to minor technical
deficiencies or momentary dropouts in the recording system or to a large number
of simultaneous cockpit/radio transmissions that obscure each other.
Fair Quality The majority of the crew conversations were intelligible. The transcript that was
developed may indicate passages where conversations were unintelligible or
fragmented. This type of recording is usually caused by cockpit noise that
obscures portions of the voice signals or by a minor electrical or mechanical
failure of the CVR system that distorts or obscures the audio information.
Poor Quality Extraordinary means had to be used to make some of the crew conversations
intelligible. The transcript that was developed may indicate fragmented phrases
and conversations and may indicate extensive passages where conversations
were missing or unintelligible. This type of recording is usually caused by a
combination of a high cockpit noise level with a low voice signal (poor signal-to-
noise ratio) or by a mechanical or electrical failure of the CVR system that
severely distorts or obscures the audio information.
Unusable Crew conversations may be discerned, but neither ordinary nor extraordinary
means made it possible to develop a meaningful transcript of the conversations.
This type of recording is usually caused by an almost total mechanical or
electrical failure of the CVR system.

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:10:52
START OF RECORDING
START OF TRANSCRIPT
04:13:04
HOT
[sound of click]
04:14:08
CTR
Empire eighty two eighty four.
04:14:10
RDO-1
go ahead.
04:14:11
CTR
Empire eighty two eighty four they said that just about anything in use
except for the uh back course. winds are out of the north. eight two
six runways are closed uh but I couldn't get a definite answer out of
them.
04:14:27
RDO-1
eight and two six are closed?
04:14:30
CTR
Empire eighty two eighty four that's what he said.
04:14:34
HOT-2
huh...so that leaves—.
04:14:38
RDO-1
pretty much leaves the runway three five left.
04:14:40
HOT-2
one seven right.
04:14:41
CTR
Empire eighty two eighty four roger.
04:14:45
HOT-2
yeah.
04:14:45
HOT-1
yeah except for he says the winds are out of the north.
96

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:14:48
HOT-2
yeah but he said that their back course isn't an option which is the only
runway— the only approach for three five.
04:14:55
HOT-1
what's that? oh. that is. oh.
04:14:59
HOT-1
well it looks like one seven left— right is the only thing available then.
04:15:03
HOT-2
that's what it sounded like but he didn't really sound like he uh knew all
that much either. [sound of laughter]
04:15:08
HOT-1
yeah.
04:15:13
HOT-1
two ninteen it looks like for the—.
04:15:17
HOT-2
for POLLO.
04:16:28
HOT-2
aw crap.
04:16:29
HOT-1
what?
04:16:30
HOT-2
I uh screwed up. I always do that...RNAV NAV.
04:18:10
HOT-2
alright I guess we can go ahead and start down.
04:18:12
HOT-1
alright.
04:18:17
RDO-1
Empire eighty two eighty four is vacating uh one four thousand for
eight thousand.
97
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:18:22
CTR
Empire eighty two eighty four roger.
04:18:43
HOT-2
alright so descent checklist.
04:18:46
HOT-1
yup. comin' right up.
04:18:52
HOT-1
uh descent...uh anti-ice is on level three. altimeters three zero one three
on the left.
04:19:00
HOT-2
on right.
04:19:00
HOT-1
CCAS is clear. belts and harnesses?
04:19:04
HOT-2
on right.
04:19:05
HOT-1
on the left. descent check complete. approach check. landing lights are
on uh cabin altitude is set and looks like it's descending nicely over there.
flight instruments and radios?
04:19:20
HOT-2
so you're gonna do this?
04:19:22
HOT-1
want me to do it?
04:19:23
HOT-2
sure.
04:19:24
HOT-1
alright. be mine the ILS we'll get vectors over to it and it's gonna beeee
the thirty three card. one oh six is the icing speed...one oh six one
twelve...uh twenty three and forty three.
98

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:19:51
HOT-1
in the event of a miss it'll be uh climb to thirty seven and a right turn to five
hundred feet via the Lubbock one fourteen radial to HYDRO intersection
and hold annnd that looks like a parallel entry.
04:20:17
HOT-2
sounds good to me.
04:20:21
HOT-1
climb to thirty seven and a left turn to five out to one fourteen. alright very
good. uh questions comments?
04:20:28
HOT-2
acceleration altitude?
04:20:31
HOT-1
uhh.
04:20:33
HOT-2
one seven— where are we? right will be thirty eight eighty.
04:20:38
HOT-1
what is it?
04:20:39
HOT-2
thirty eight eighty.
04:20:39
HOT-1
thirty eight eighty. okay very good.
04:21:02
HOT-2
[sound similar to yawning]
04:21:19
HOT-1
and uh descent approach check is complete.
04:21:24
HOT-2
roger.
04:22:06
CTR
Empire eighty two eighty four contact Lubbock Approach one one niner
point two.
99

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:22:11
RDO-1
ninteen two Empire eighty two eighty four good morning.
04:22:16
HOT
[sound similar to frequency change tone]
04:22:19
RDO-1
morning Lubbock Empire eighty two eighty four is out of one zero
thousand for eight thousand.
04:22:25
APP
Empire eighty two eighty four Lubbock Approach. [sound of tone]
04:22:29
HOT-1
yup. he needs to answer that phone.
04:22:32
APP
Empire eighty two eighty four Lubbock Approach descend at pilot's
discretion maintain six thousand. I haven't had any icing reports.
special weather observation at uh one zero zero eight Zulu. wind three
five zero at one zero visibility two. light freezing drizzle mist. ceiling
five hundred overcast. temperature minus eight dewpoint minus niner.
altimeter three zero one two. advise uh braking action advisories are
in effect. advise what approach you'd want. runway eight two six is
closed.
04:23:05
RDO-1
well that pretty much uh leaves us with one seven right sir.
04:23:14
APP
Empire eighty two eighty four expect ILS runway one seven right.
04:23:17
RDO-1
roger that.
04:23:19
HOT-1
uh—.
04:23:19
HOT-2
right.
04:23:21
HOT-1
two miles five hundred feet.
100
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:23:22
HOT-2
yeah I can do it then.
04:23:23
HOT-1
yup all yours.
04:23:24
HOT-2
cool.
04:23:33
HOT-2
uh uh did you call—.
04:23:33
APP
Empire eighty two eighty four mu readings for runway three five left
were twenty four twenty five twenty three.
04:23:40
RDO-1
roger.
04:23:48
HOT-2
what was that he just said?
04:23:50
HOT-1
RVR?
04:23:51
HOT-2
oh RVR.
04:23:51
HOT-1
did he say RVR reading?
04:23:54
HOT-2
he said something. I— I didn't catch what he said.
04:23:58
APP
Empire eighty two eighty four fly heading two niner zero vector for the
approach.
04:24:02
RDO-1
two nine zero Empire eighty two eighty four and what was that
touchdown zone RVR you said again?
101

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:24:08
APP
well RVR's more than six thousand runway one seven right. and the
mu readings for runway three five left touchdown twenty four. midpoint
uh twenty five. rollout twenty three.
04:24:21
RDO-1
okay very good. I got you now.
04:24:23
HOT-2
what is it? m—.
04:24:24
HOT-1
oh it's the braking action yeah.
04:24:25
HOT-2
oh braking action.
04:24:27
HOT-2
I got ya. um.
04:24:30
HOT-1
yeah when we get down there just don't do anything like— just keep it
going down the center line of the runway. and don't be touching any
brakes and make sure that we get two low pitch stops.
04:24:39
HOT-2
okay.
04:24:40
HOT-1
yeah.
04:24:43
HOT-2
did you call ops yet?
04:24:45
HOT-1
no I didn't. uh they're on thirty one ninety two?
04:24:49
HOT-2
yeah.
04:24:51
HOT-2
that's the normal one isn't it? yeah that's it.
102
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:24:53
HOT-1
yeah.
04:24:57
RDO-1
ops eighty two eighty four is like fifteen minutes out.
04:25:13
RDO-1
Lubbock ops eighty two eighty four.
04:25:17
OPS
go ahead eighty two eighty four this is Lubbock.
04:25:17
HOT
[sound similar to altitude alert]
04:25:19
RDO-1
yup uh we're like fifteen minutes out.
04:25:22
OPS
copy that uh eighty two eighty four. we didn't think you guys were
comin' in. uh do you know if you 'll be able to depart?
04:25:29
RDO-1
okay uh part of that is broken and unreadable. say again.
04:25:34
OPS
I said we didn't think you guys were coming in this morning. you know
if uh you guys are gonna be able to depart?
04:25:40
RDO-1
you got deicing right?
04:25:43
OPS
yeah ten four.
04:25:44
RDO-1
well we don't know yet. we're gonna have to talk about it when we get
on the ground.
04:25:49
OPS
okey doke well we'll see you guys in about fifteen minutes.
103
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:25:52
RDO-1
roger that.
04:25:53
HOT-1
good grief.
04:25:54
HOT-2
do they have icing?
04:25:55
HOT-1
well she says oh we didn't know that you guys were coming. I'm thinking
doesn't— doesn't AFW— I mean didn't I call back the numbers?
04:25:58
HOT-2
[sound of laughter]
04:26:03
HOT-2
yeah...huh...that's great...does that mean we can just go straight to uh
Midland? [sound of laughter]
04:26:14
HOT-1
don't we wish.
04:26:18
HOT-1
oh we didn't know you were coming. oh for Gods sake.
04:26:23
HOT-2
exactly.
04:26:30
HOT-1
let's see since we're on a heading we'll go with this. and one oh nine two.
04:26:37
HOT-2
that's the...Midland VOR. so thirteen—.
04:26:42
HOT-1
it is—.
04:26:43
HOT-2
where are we here?
04:26:45
HOT-1
uh it is one oh nine five.
104
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:26:47
HOT-2
one oh nine five for the localizer.
04:26:51
HOT-1
there we go.
04:26:53
HOT-2
one oh nine five set.
04:26:56
HOT-1
and we'll put in—. it is—.
04:27:01
HOT-2
POLLO.
04:27:02
HOT-1
it is I-L-B-B.
04:27:07
HOT-2
cool.
04:27:26
HOT-1
it's like four miles or something. five point five. I'll buy that.
04:27:34
HOT-1
let's see— we're oh we're on heading now right?
04:27:35
HOT-2
we're on heading yeah.
04:27:40
HOT-1
and...what is it uh one seventy two.
04:27:44
HOT-2
and.
04:28:00
HOT-2
very good thank you.
04:28:01
HOT-1
you're welcome.
105
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:28:08
HOT-1
what was that one burp? was that a big chunk of ice going into one of our
quality Pratt & Whitney one hundreds out there?
04:28:14
HOT-2
that's what I'm guessing it was. [sound of laughter]
04:28:17
HOT-1
nice. let's see—.
04:28:20
HOT-2
that was a little strange.
04:28:21
HOT-1
yeah *.
04:28:51
HOT-2
alright.
04:29:13
HOT-1
yeah one of the guys told me one time that he was here in Lubbock and it
was snowing.
04:29:18
HOT-2
weird.
04:29:35
APP
Empire eighty two eighty four dec— descend and maintain five
thousand.
04:29:38
RDO-1
five thousand eighty two eighty four.
04:29:43
HOT-2
five thousand set.
04:29:48
HOT
[sound similar to altitude alert]
04:29:51
HOT-1
one to go.
106

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:29:52
HOT-2
one to go.
04:30:15
HOT
[sound similar to master caution single chime]
04:30:21
HOT-1
wow that was a hell of a change.
04:30:23
HOT-2
no kidding.
04:30:35
APP
Empire eighty two eighty four turn left heading two six zero.
04:30:36
HOT
[sound similar to altitude alert]
04:30:38
RDO-1
two six zero eighty two eighty four.
04:30:41
HOT-2
two six zero...ALT star.
04:30:48
HOT-1
two six zero.
04:31:25
APP
Empire eighty two eighty four turn right heading two eight zero.
04:31:29
RDO-1
two eight zero eighty two eighty four.
04:31:33
APP
wind change between six and five thousand from the south to the
north.
04:31:36
HOT-2
hah.
04:31:37
RDO-1
roger.
107
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:31:39
RDO-1
yeah the uh the temperature actually uh dropped uh 'bout eight
degrees in that amount of time as well.
04:31:47
APP
yeah you were— you had a— at six thousand you had a south wind
blowin' about fifteen degrees to the north and er pushing you off that
g— off course that much and when at five thousand it went exactly the
opposite.
04:32:01
RDO-1
we concur.
04:32:02
HOT-2
[sound of laughter]
04:32:07
HOT-2
my goodness.
04:32:19
RDO-1
when they sent me down here they said that I would uh I'd find things
unusual.
04:32:24
APP
that's— that's west Texas weather for sure.
04:32:27
HOT-2
[sound of laughter]
04:32:51
HOT-2
can you ID it for me really quick?
04:32:53
HOT-1
yeah.
04:32:53
HOT-2
thanks.
108

INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:33:00
I-LBB
[sound of I-LBB morse code identifier]
04:33:04
APP
Empire eighty two eighty four turn seven miles from the outer marker.
turn left heading two one zero. maintain five thousand until established
on the localizer. cleared ILS runway one seven right approach.
04:33:13
RDO-1
five thousand two ten until established and cleared for the ILS Empire
eighty two eighty four.
04:33:19
HOT-1
you are cleared for the approach and you are identified.
04:33:21
HOT-2
approach...alright thank you.
04:33:26
I-LBB
[sound of I-LBB morse code identifier]
04:33:33
HOT-1
course alive on the left.
04:33:35
HOT-2
LOC star.
04:33:35
HOT-1
and you're ten miles out. we probably better get this thing uh squared
away here.
04:33:39
HOT-2
okay.
04:33:41
HOT-1
annnnd there we go.
04:33:44
HOT-2
alright.
04:33:52
APP
Empire eighty two eighty four contact tower one two zero point five.
109
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:33:55
RDO-1
twenty point five thanks a lot. we'll see you on the way out.
04:33:58
APP
roger.
04:33:59
HOT
[sound similar to frequency change tone]
04:34:01
RDO-1
Empire eighty two eighty four is uh checkin' in nine out on the localizer
inbound.
04:34:06
TWR
Empire eighty two eighty four Lubbock Tower runway one seven right
clear to land. winds zero one ze ro at eight.
04:34:11
RDO-1
roger clear to land.
04:34:14
HOT-2
alright...go.
04:34:24
HOT-2
flaps fifteen gear down landing check.
04:34:29
CAM
[sound similar to landing gear deployment]
04:34:33
HOT-1
alright awww landing check. start selector is continuous relight. power
management is in takeoff. icing AOA is on landing gear confirmed three
green.
04:34:43
HOT-2
glideslope star.
04:34:48
HOT-2
confirmed.
04:34:48
HOT-1
uh let's see we should have glideslope star.
110
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:34:52
HOT-2
*.
04:34:52
HOT-1
very good...and flaps condition levers to go.
04:34:58
HOT
[sound similar to altitude alert]
04:34:58
HOT-2
alright ah dangit.
04:35:01
HOT
[sound of 0.3 second duration whistle increasing frequency from
approximately 835 to 1050 Hz]
04:35:03
HOT-2
what the heck is going on?
04:35:04
HOT-1
you know what? we have no flaps.
04:35:08
HOT-2
aw #.
04:35:09
HOT-1
#.
04:35:10
LB
[sound similar to outer marker]
04:35:15
CAM
[sound of click]
04:35:16
HOT-1
uhh.
04:35:19
HOT-2
*.
04:35:22
TAWS
one thousand.
111
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:35:23
HOT-2
okay.
04:35:28
HOT-1
what the hell?
04:35:30
HOT
[sound similar to stall warning and stickshaker lasting 1.1 seconds]
04:35:31
HOT-2
aw #.
04:35:31
HOT-1
yeah don't do that.
04:35:32
CAM
[sound similar to stall warning lasting 0.3 seconds]
04:35:34
HOT-2
alright.
04:35:36
HOT-1
just keep flying the airplane. okay.
04:35:40
HOT-2
should I go around?
04:35:41
HOT-1
no.
04:35:41
TWR
winds zero one zero at eight.
04:35:43
HOT-1
keep descending.
04:35:44
HOT-2
we're getting pretty close here. [straining]
04:35:45
HOT-1
what's that? you want me to finish it?
112
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:35:47
HOT-2
yes please.
04:35:48
HOT-1
okay my airplane.
04:35:49
HOT-2
your controls.
04:35:50
HOT-?
[sound of heavy breathing]
04:35:52
HOT-2
alright you got power.
04:35:53
HOT
[sound similar to altitude alert]
04:35:58
TAWS
five hundred.
04:36:00
HOT-1
aw #.
04:36:00
HOT
[sound similar to stall warning and stickshaker lasting 0.9 seconds]
04:36:00
TAWS
pull up. pull up.
04:36:02
HOT-1
okay.
04:36:04
HOT-2
there's the runway.
04:36:15
HOT-2
alright your—.
04:36:17
HOT-1
max RPM.
113
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
04:36:17
HOT-2
max RPM.
04:36:19
CAM
[sound similar to RPM increase]
04:36:19
HOT
[sound similar to stall warning and stickshaker lasting 0.5 seconds]
04:36:20
HOT
[sound similar to stall warning and stickshaker lasting 5.4 seconds]
04:36:22
HOT-2
oh #.
04:36:25
HOT-1
#.
04:36:25
HOT-2
#. [straining]
04:36:26
CAM
[sound of beep]
04:36:27
CAM
[sound of impact]
04:36:28
CAM
[sound of grinding and scraping]
04:36:29
CAM
[sound similar to stall warning]
04:36:32
CAM
[sound of continuous repetitive chime continues until end of recording]
04:36:43
CAM
[sound similar to occupants moving around in cockpit]
04:36:45
HOT-1
get out of the airplane. get out of the airplane.
114
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
115
04:36:48
CAM
[sound of scraping stops]
04:36:52
CAM-1
go out the— go out the hatch.
04:37:10
CAM-1
there's a fire on the right hand side. go out the left.
04:37:16
CAM-1
no you know what—.
04:37:17
CAM-2
what.
04:37:17
CAM-1
when you get out can you get out—.
04:37:25
CAM
[sound similar to door opening]
04:37:27
CAM-1
*.
04:41:35
END OF TRANSCRIPT
END OF RECORDING
